Risk factors for metachronous colorectal cancer or advanced lesions after endoscopic resection of serrated polyps: a systematic review and meta-analysis
{"title":"Risk factors for metachronous colorectal cancer or advanced lesions after endoscopic resection of serrated polyps: a systematic review and meta-analysis","authors":"","doi":"10.1016/j.gie.2024.05.021","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and Aims</h3><div>Serrated polyps (SPs) are precursors to 15% to 20% of colorectal cancers (CRCs). However, there are uncertainties regarding which SPs require surveillance and at what intervals, with recommendations adapted from those for adenomas in the absence of solid evidence. Our aim was to assess which SP risk characteristics relate to a higher risk of metachronous CRC or advanced polyps.</div></div><div><h3>Methods</h3><div>We systematically searched PubMed, Embase, and Cochrane for cohort studies, case-control studies, and clinical trials from inception to December 31, 2023, of CRC or advanced polyps (advanced adenoma [AA] or advanced SP) incidence at surveillance stratified by baseline SP size, dysplasia, location, and multiplicity. We defined advanced SPs as those ≥10 mm or with dysplasia. CRC and advanced polyp incidence per 1000 person-years were estimated. We performed a meta-analysis by calculating pooled relative risks (RRs) using a random-effects model.</div></div><div><h3>Results</h3><div>A total of 5903 studies were reviewed, and 14 were included with 493,949 patients (mean age, 59.5 years; 55% men). The mean follow-up was 4.9 years. CRC incidence per 1000 person-years was 2.09 (95% confidence interval [CI], 1.29-2.90) for advanced SPs, 1.52 (95% CI, 0.78-2.25) for SPs of ≥10 mm, 5.86 (95% CI, 2.16-9.56) for SPs with dysplasia, 1.18 (95% CI, 0.77-1.60) for proximal SPs, 0.52 (95% CI, 0.08-1.12) for ≥3 SPs, 0.50 (95% CI, 0.35-0.66) for nonadvanced SPs, and 0.44 (95% CI, 0.41-0.46) for normal colonoscopy findings. Metachronous CRC risk was higher in advanced SPs versus nonadvanced SPs (RR, 1.84; 95% CI, 1.11-3.04) and versus normal colonoscopy findings (RR, 2.92; 95% CI, 2.26-3.77), in SPs of ≥10 mm versus <10 mm (RR, 2.61; 95% CI, 1.43-4.77) and versus normal colonoscopy findings (RR: 3.52; 95% CI, 2.17-5.69); and in SPs with dysplasia versus normal colonoscopy findings (RR: 2.71; 95% CI, 2.00-3.67). No increase in CRC or advanced polyp risk was found in patients with proximal versus distal SPs, nor in ≥3 SPs versus 1 or 2 SPs.</div></div><div><h3>Conclusions</h3><div>CRC risk is significantly higher in patients with baseline advanced SPs after 4.9 years of follow-up, with risk magnitudes similar to those described for AA, supporting the current recommendation for 3-year surveillance in patients with advanced SPs.</div></div>","PeriodicalId":12542,"journal":{"name":"Gastrointestinal endoscopy","volume":"100 4","pages":"Pages 605-615.e14"},"PeriodicalIF":7.5000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastrointestinal endoscopy","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0016510724032577","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and Aims
Serrated polyps (SPs) are precursors to 15% to 20% of colorectal cancers (CRCs). However, there are uncertainties regarding which SPs require surveillance and at what intervals, with recommendations adapted from those for adenomas in the absence of solid evidence. Our aim was to assess which SP risk characteristics relate to a higher risk of metachronous CRC or advanced polyps.
Methods
We systematically searched PubMed, Embase, and Cochrane for cohort studies, case-control studies, and clinical trials from inception to December 31, 2023, of CRC or advanced polyps (advanced adenoma [AA] or advanced SP) incidence at surveillance stratified by baseline SP size, dysplasia, location, and multiplicity. We defined advanced SPs as those ≥10 mm or with dysplasia. CRC and advanced polyp incidence per 1000 person-years were estimated. We performed a meta-analysis by calculating pooled relative risks (RRs) using a random-effects model.
Results
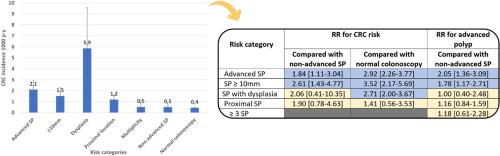
A total of 5903 studies were reviewed, and 14 were included with 493,949 patients (mean age, 59.5 years; 55% men). The mean follow-up was 4.9 years. CRC incidence per 1000 person-years was 2.09 (95% confidence interval [CI], 1.29-2.90) for advanced SPs, 1.52 (95% CI, 0.78-2.25) for SPs of ≥10 mm, 5.86 (95% CI, 2.16-9.56) for SPs with dysplasia, 1.18 (95% CI, 0.77-1.60) for proximal SPs, 0.52 (95% CI, 0.08-1.12) for ≥3 SPs, 0.50 (95% CI, 0.35-0.66) for nonadvanced SPs, and 0.44 (95% CI, 0.41-0.46) for normal colonoscopy findings. Metachronous CRC risk was higher in advanced SPs versus nonadvanced SPs (RR, 1.84; 95% CI, 1.11-3.04) and versus normal colonoscopy findings (RR, 2.92; 95% CI, 2.26-3.77), in SPs of ≥10 mm versus <10 mm (RR, 2.61; 95% CI, 1.43-4.77) and versus normal colonoscopy findings (RR: 3.52; 95% CI, 2.17-5.69); and in SPs with dysplasia versus normal colonoscopy findings (RR: 2.71; 95% CI, 2.00-3.67). No increase in CRC or advanced polyp risk was found in patients with proximal versus distal SPs, nor in ≥3 SPs versus 1 or 2 SPs.
Conclusions
CRC risk is significantly higher in patients with baseline advanced SPs after 4.9 years of follow-up, with risk magnitudes similar to those described for AA, supporting the current recommendation for 3-year surveillance in patients with advanced SPs.
期刊介绍:
Gastrointestinal Endoscopy is a journal publishing original, peer-reviewed articles on endoscopic procedures for studying, diagnosing, and treating digestive diseases. It covers outcomes research, prospective studies, and controlled trials of new endoscopic instruments and treatment methods. The online features include full-text articles, video and audio clips, and MEDLINE links. The journal serves as an international forum for the latest developments in the specialty, offering challenging reports from authorities worldwide. It also publishes abstracts of significant articles from other clinical publications, accompanied by expert commentaries.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
