Left ventricular unloading via percutaneous assist device during extracorporeal membrane oxygenation in acute myocardial infarction and cardiac arrest.
Jake M Kieserman, Ivan A Kuznetsov, Joseph Park, James W Schurr, Omar Toubat, Salim Olia, Christian Bermudez, Marisa Cevasco, Joyce Wald
{"title":"Left ventricular unloading via percutaneous assist device during extracorporeal membrane oxygenation in acute myocardial infarction and cardiac arrest.","authors":"Jake M Kieserman, Ivan A Kuznetsov, Joseph Park, James W Schurr, Omar Toubat, Salim Olia, Christian Bermudez, Marisa Cevasco, Joyce Wald","doi":"10.1177/03913988241254978","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>A feared complication of an acute myocardial infarction (AMI) is cardiac arrest (CA). Even if return of spontaneous circulation is achieved, cardiogenic shock (CS) is common. Venoarterial extracorporeal membrane oxygenation (VA-ECMO) supports patients with CS and is often used in conjunction with an Impella device (2.5 and CP) to off-load the left ventricle, although limited evidence supports this approach.</p><p><strong>Methods: </strong>The goal of this study was to determine whether a mortality difference was observed in VA-ECMO alone versus VA-ECMO with Impella (ECPELLA) in patients with CS from AMI and CA. A retrospective chart review of 50 patients with AMI-CS and CA and were supported with VA-ECMO (<i>n</i> = 34) or ECPELLA (<i>n</i> = 16) was performed. The primary outcome was all-cause mortality at 6-months from VA-ECMO or Impella implantation. Secondary outcomes included in-hospital mortality and complication rates between both cohorts and intensive care unit data.</p><p><strong>Results: </strong>Baseline characteristics were similar, except patients with ST-elevation myocardial infarction were more likely to be in the VA-ECMO group (<i>p</i> = 0.044). The ECPELLA cohort had significantly worse survival after VA-ECMO (SAVE) score (<i>p</i> = 0.032). Six-month all-cause mortality was not significantly different between the cohorts, even when adjusting for SAVE score. Secondary outcomes were notable for an increased rate of minor complications without an increased rate of major complications in the ECPELLA group.</p><p><strong>Conclusions: </strong>Randomized trials are needed to determine if a mortality difference exists between VA-ECMO and ECPELLA platforms in patients with AMI complicated by CA and CS.</p>","PeriodicalId":13932,"journal":{"name":"International Journal of Artificial Organs","volume":" ","pages":"401-410"},"PeriodicalIF":1.3000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11826357/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Artificial Organs","FirstCategoryId":"5","ListUrlMain":"https://doi.org/10.1177/03913988241254978","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/10 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: A feared complication of an acute myocardial infarction (AMI) is cardiac arrest (CA). Even if return of spontaneous circulation is achieved, cardiogenic shock (CS) is common. Venoarterial extracorporeal membrane oxygenation (VA-ECMO) supports patients with CS and is often used in conjunction with an Impella device (2.5 and CP) to off-load the left ventricle, although limited evidence supports this approach.
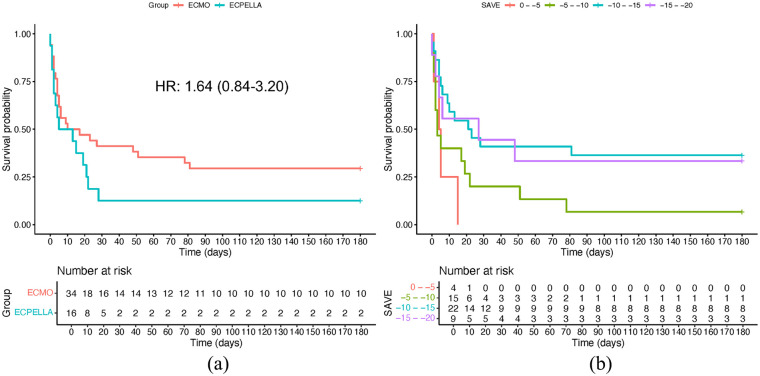
Methods: The goal of this study was to determine whether a mortality difference was observed in VA-ECMO alone versus VA-ECMO with Impella (ECPELLA) in patients with CS from AMI and CA. A retrospective chart review of 50 patients with AMI-CS and CA and were supported with VA-ECMO (n = 34) or ECPELLA (n = 16) was performed. The primary outcome was all-cause mortality at 6-months from VA-ECMO or Impella implantation. Secondary outcomes included in-hospital mortality and complication rates between both cohorts and intensive care unit data.
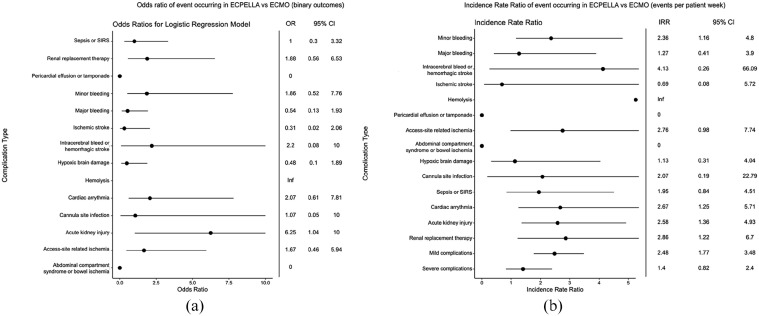
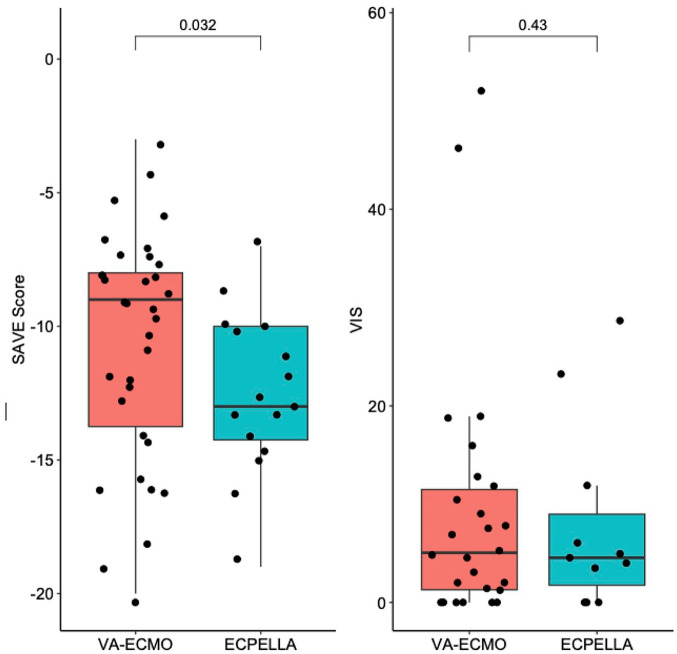
Results: Baseline characteristics were similar, except patients with ST-elevation myocardial infarction were more likely to be in the VA-ECMO group (p = 0.044). The ECPELLA cohort had significantly worse survival after VA-ECMO (SAVE) score (p = 0.032). Six-month all-cause mortality was not significantly different between the cohorts, even when adjusting for SAVE score. Secondary outcomes were notable for an increased rate of minor complications without an increased rate of major complications in the ECPELLA group.
Conclusions: Randomized trials are needed to determine if a mortality difference exists between VA-ECMO and ECPELLA platforms in patients with AMI complicated by CA and CS.
期刊介绍:
The International Journal of Artificial Organs (IJAO) publishes peer-reviewed research and clinical, experimental and theoretical, contributions to the field of artificial, bioartificial and tissue-engineered organs. The mission of the IJAO is to foster the development and optimization of artificial, bioartificial and tissue-engineered organs, for implantation or use in procedures, to treat functional deficits of all human tissues and organs.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
