Maximilian Grummt, Lorena Hafermann, Lars Claussen, Carolin Herrmann, Bernd Wolfarth
{"title":"Rating of Perceived Exertion: A Large Cross-Sectional Study Defining Intensity Levels for Individual Physical Activity Recommendations.","authors":"Maximilian Grummt, Lorena Hafermann, Lars Claussen, Carolin Herrmann, Bernd Wolfarth","doi":"10.1186/s40798-024-00729-1","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Physical inactivity is a growing risk factor worldwide, therefore getting people into sports is necessary. When prescribing physical activity, it is essential to recommend the correct training intensities. Cardiopulmonary exercise testing (CPX) enables precise determination of individuals' training intensities but is unavailable for a broad population. Therefore, the Borg scale allows individuals to assess perceived exertion and set their intensity easily and cost-efficiently. In order to transfer CPX to rating of perceived exertion (RPE), previous studies investigated RPE on specific physiological anchors, e.g. blood lactate (bLa) concentrations, but representativeness for a broad population is questionable. Some contradictory findings regarding individual factors influencing RPE occur, whereas univariable analysis has been performed so far. Moreover, a multivariable understanding of individual factors influencing RPE is missing. This study aims to determine RPE values at the individual anaerobic threshold (LT2) and defined bLa concentrations in a large cohort and to evaluate individual factors influencing RPE with multivariable analysis.</p><p><strong>Methods: </strong>CPX with bicycle or treadmill ergometer of 6311 participants were analyzed in this cross-sectional study. RPE values at bLa concentrations 2 mmol/l, 3 mmol/l, 4 mmol/l, and LT2 (first rise in bLa over baseline + 1.5 mmol/l) were estimated by spline interpolation. Multivariable cumulative ordinal regression models were performed to assess the influence of sex, age, type of ergometry, VO2max, and duration of exercise testing on RPE.</p><p><strong>Results: </strong>Median values [interquartile range (IQR)] of the total population were RPE 13 [11; 14] at 2 mmol/l, RPE 15 [13; 16] at 3 mmol/l, RPE 16 [15; 17] at 4 mmol/l, and RPE 15 [14; 16] at LT2. Main influence of individual factors on RPE were seen especially at 2 mmol/l: male sex (odds ratio (OR) [95%-CI]: 0.65 [0.587; 0.719]), treadmill ergometry (OR 0.754 [0.641; 0.886]), number of stages (OR 1.345 [1.300; 1.394]), age (OR 1.015 [1.012; 1.018]), and VO2max (OR 1.023 [1.015; 1.030]). Number of stages was the only identified influencing factor on RPE at all lactate concentrations/LT2 (3 mmol/l: OR 1.290 [1.244; 1.336]; 4 mmol/l: OR 1.229 [1.187; 1.274]; LT2: OR 1.155 [1.115; 1.197]).</p><p><strong>Conclusion: </strong>Our results suggest RPE ≤ 11 for light intensity, RPE 12-14 for moderate intensity, and RPE 15-17 for vigorous intensity, which slightly differs from the current American College of Sports Medicine (ACSM) recommendations. Additionally, we propose an RPE of 15 delineating heavy and severe intensity domain. Age, sex, type of ergometry, duration of exercise, and cardiopulmonary fitness should be considered when recommending individualized intensities with RPE, primarily at lower intensities. Therefore, this study can be used as a new guideline for prescribing individual RPE values in the clinical practice, predominantly for endurance type exercise.</p>","PeriodicalId":21788,"journal":{"name":"Sports Medicine - Open","volume":"10 1","pages":"71"},"PeriodicalIF":5.9000,"publicationDate":"2024-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11164849/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Sports Medicine - Open","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40798-024-00729-1","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SPORT SCIENCES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Physical inactivity is a growing risk factor worldwide, therefore getting people into sports is necessary. When prescribing physical activity, it is essential to recommend the correct training intensities. Cardiopulmonary exercise testing (CPX) enables precise determination of individuals' training intensities but is unavailable for a broad population. Therefore, the Borg scale allows individuals to assess perceived exertion and set their intensity easily and cost-efficiently. In order to transfer CPX to rating of perceived exertion (RPE), previous studies investigated RPE on specific physiological anchors, e.g. blood lactate (bLa) concentrations, but representativeness for a broad population is questionable. Some contradictory findings regarding individual factors influencing RPE occur, whereas univariable analysis has been performed so far. Moreover, a multivariable understanding of individual factors influencing RPE is missing. This study aims to determine RPE values at the individual anaerobic threshold (LT2) and defined bLa concentrations in a large cohort and to evaluate individual factors influencing RPE with multivariable analysis.
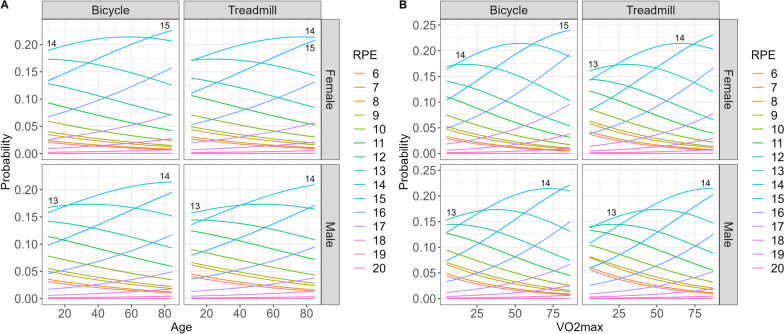
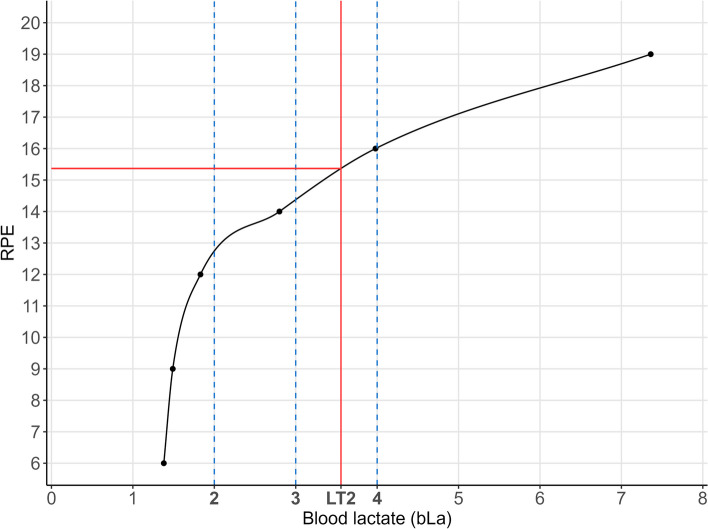
Methods: CPX with bicycle or treadmill ergometer of 6311 participants were analyzed in this cross-sectional study. RPE values at bLa concentrations 2 mmol/l, 3 mmol/l, 4 mmol/l, and LT2 (first rise in bLa over baseline + 1.5 mmol/l) were estimated by spline interpolation. Multivariable cumulative ordinal regression models were performed to assess the influence of sex, age, type of ergometry, VO2max, and duration of exercise testing on RPE.
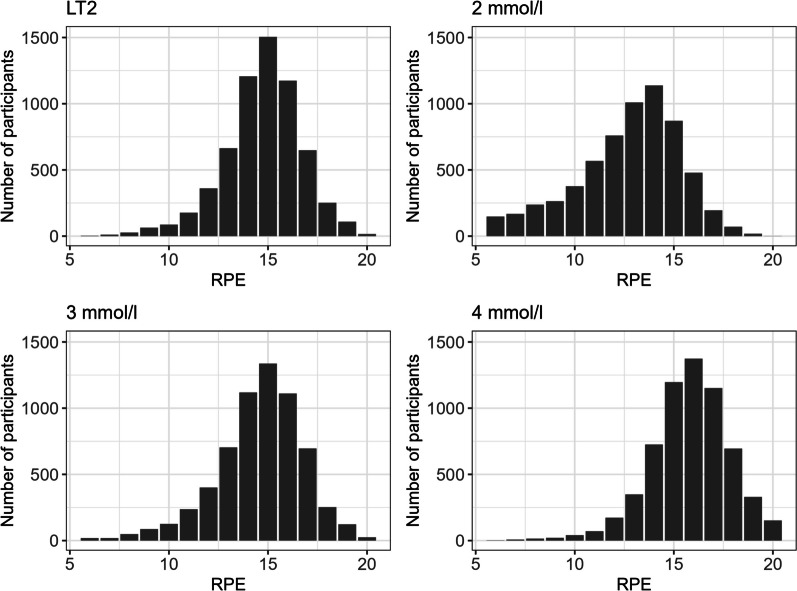
Results: Median values [interquartile range (IQR)] of the total population were RPE 13 [11; 14] at 2 mmol/l, RPE 15 [13; 16] at 3 mmol/l, RPE 16 [15; 17] at 4 mmol/l, and RPE 15 [14; 16] at LT2. Main influence of individual factors on RPE were seen especially at 2 mmol/l: male sex (odds ratio (OR) [95%-CI]: 0.65 [0.587; 0.719]), treadmill ergometry (OR 0.754 [0.641; 0.886]), number of stages (OR 1.345 [1.300; 1.394]), age (OR 1.015 [1.012; 1.018]), and VO2max (OR 1.023 [1.015; 1.030]). Number of stages was the only identified influencing factor on RPE at all lactate concentrations/LT2 (3 mmol/l: OR 1.290 [1.244; 1.336]; 4 mmol/l: OR 1.229 [1.187; 1.274]; LT2: OR 1.155 [1.115; 1.197]).
Conclusion: Our results suggest RPE ≤ 11 for light intensity, RPE 12-14 for moderate intensity, and RPE 15-17 for vigorous intensity, which slightly differs from the current American College of Sports Medicine (ACSM) recommendations. Additionally, we propose an RPE of 15 delineating heavy and severe intensity domain. Age, sex, type of ergometry, duration of exercise, and cardiopulmonary fitness should be considered when recommending individualized intensities with RPE, primarily at lower intensities. Therefore, this study can be used as a new guideline for prescribing individual RPE values in the clinical practice, predominantly for endurance type exercise.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
