Sandon Scott, Brennan Morrison, Kate Young, Lauren Clark, Yanming Li, Carissa Walter, Aaron Rohr, Adam Alli
{"title":"Re-expansion Pulmonary Edema (REPE) Following Thoracentesis: Is Large-Volume Thoracentesis Associated with Increased Incidence of REPE?","authors":"Sandon Scott, Brennan Morrison, Kate Young, Lauren Clark, Yanming Li, Carissa Walter, Aaron Rohr, Adam Alli","doi":"10.1007/s00270-024-03773-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To determine the safety and efficacy associated with drainage volumes greater than 1,500 mL in a single, unilateral thoracentesis without pleural manometry measurements.</p><p><strong>Materials and methods: </strong>This retrospective, single-institution study included 872 patients (18 years and older) who underwent ultrasound-guided thoracentesis. Patient and procedures data were collected including demographics, number of and laterality of thoracenteses, volume and consistency of fluid removed, and whether clinical or radiologic evidence of re-expansion pulmonary edema (REPE) developed within 24 h of thoracentesis. Fisher's exact test was used to test the significance of the relationship between volume of fluid removed and evidence of REPE.</p><p><strong>Results: </strong>A total of 1376 thoracenteses were performed among the patients included in the study. The mean volume of fluid removed among all procedures was 901.1 mL (SD = 641.7 mL), with 194 (14.1%) procedures involving the removal of ≥ 1,500 mL of fluid. In total, six (0.7%) patients developed signs of REPE following thoracentesis, five of which were a first-time thoracentesis. No statistically significant difference in incidence of REPE was observed between those with ≥ 1,500 mL of fluid removed compared to those with < 1,500 mL of fluid removed (p-value = 0.599).</p><p><strong>Conclusions: </strong>Large-volume thoracentesis may safely improve patients' symptoms while preventing the need for repeat procedures.</p>","PeriodicalId":9591,"journal":{"name":"CardioVascular and Interventional Radiology","volume":null,"pages":null},"PeriodicalIF":2.8000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CardioVascular and Interventional Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00270-024-03773-2","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To determine the safety and efficacy associated with drainage volumes greater than 1,500 mL in a single, unilateral thoracentesis without pleural manometry measurements.
Materials and methods: This retrospective, single-institution study included 872 patients (18 years and older) who underwent ultrasound-guided thoracentesis. Patient and procedures data were collected including demographics, number of and laterality of thoracenteses, volume and consistency of fluid removed, and whether clinical or radiologic evidence of re-expansion pulmonary edema (REPE) developed within 24 h of thoracentesis. Fisher's exact test was used to test the significance of the relationship between volume of fluid removed and evidence of REPE.
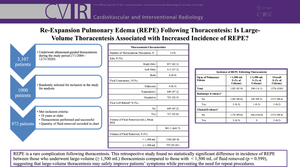
Results: A total of 1376 thoracenteses were performed among the patients included in the study. The mean volume of fluid removed among all procedures was 901.1 mL (SD = 641.7 mL), with 194 (14.1%) procedures involving the removal of ≥ 1,500 mL of fluid. In total, six (0.7%) patients developed signs of REPE following thoracentesis, five of which were a first-time thoracentesis. No statistically significant difference in incidence of REPE was observed between those with ≥ 1,500 mL of fluid removed compared to those with < 1,500 mL of fluid removed (p-value = 0.599).
Conclusions: Large-volume thoracentesis may safely improve patients' symptoms while preventing the need for repeat procedures.
期刊介绍:
CardioVascular and Interventional Radiology (CVIR) is the official journal of the Cardiovascular and Interventional Radiological Society of Europe, and is also the official organ of a number of additional distinguished national and international interventional radiological societies. CVIR publishes double blinded peer-reviewed original research work including clinical and laboratory investigations, technical notes, case reports, works in progress, and letters to the editor, as well as review articles, pictorial essays, editorials, and special invited submissions in the field of vascular and interventional radiology. Beside the communication of the latest research results in this field, it is also the aim of CVIR to support continuous medical education. Articles that are accepted for publication are done so with the understanding that they, or their substantive contents, have not been and will not be submitted to any other publication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
