Ali Husnain, Asad Malik, Juan Caicedo, Satish Nadig, Daniel Borja-Cacho, Justin Boike, Josh Levitsky, Allison Reiland, Bartley Thornburg, Rajesh Keswani, Muhammed Sufyaan Ebrahim Patel, Aziz Aadam, Riad Salem, Andres Duarte, Daniel Ganger, Ahsun Riaz
{"title":"Percutaneous Biliary Interventions via the Modified Hutson Loop in Patients with Biliary-Enteric Anastomoses: A Retrospective Study.","authors":"Ali Husnain, Asad Malik, Juan Caicedo, Satish Nadig, Daniel Borja-Cacho, Justin Boike, Josh Levitsky, Allison Reiland, Bartley Thornburg, Rajesh Keswani, Muhammed Sufyaan Ebrahim Patel, Aziz Aadam, Riad Salem, Andres Duarte, Daniel Ganger, Ahsun Riaz","doi":"10.1007/s00270-024-03778-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to present the institutional experience and algorithm for performing biliary interventions in liver transplant patients using the modified Hutson loop access (MHLA) and the impact of percutaneous endoscopy via the MHLA on these procedures.</p><p><strong>Methods: </strong>Over 13 years, 201 MHLA procedures were attempted on 52 patients (45 liver transplants; 24 living and 21 deceased donors) for diagnostic (e.g., cholangiography) and therapeutic (e.g., stent/drain insertion and cholangioplasty) purposes. The most common indications for MHLA were biliary strictures (60%) and bile leaks (23%). Percutaneous endoscopy was used to directly visualize the biliary-enteric anastomosis, diagnose pathology (e.g., ischemic cholangiopathy), and help in biliary hygiene (removing debris/casts/stones/stents) in 138/201 (69%) procedures. Technical success was defined as cannulating the biliary-enteric anastomosis and performing diagnostic/therapeutic procedure via the MHLA.</p><p><strong>Results: </strong>The technical success rate was 95% (190/201). The failure rate among procedures performed with and without endoscopy was 2% (3/138) versus 13% (8/63) (P = 0.0024), and the need for new transhepatic access (to aid the procedure) was 12% (16/138) versus 30% (19/63) (P = 0.001). Despite endoscopy, failure in 2% of the cases resulted from inflamed/friable anastomosis (1/3) and high-grade stricture (2/3) obstructing retrograde cannulation of biliary-enteric anastomosis. Major adverse events (bowel perforation and injury) occurred in 1% of the procedures, with no procedure-related mortality.</p><p><strong>Conclusions: </strong>MHLA-based percutaneous biliary intervention is a safe and effective alternative to managing complications after liver transplant. Percutaneous endoscopy via the MHLA improves success rates and may reduce the need for new transhepatic access. Level of Evidence Level 4.</p>","PeriodicalId":9591,"journal":{"name":"CardioVascular and Interventional Radiology","volume":" ","pages":"1083-1092"},"PeriodicalIF":2.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CardioVascular and Interventional Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00270-024-03778-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/10 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aimed to present the institutional experience and algorithm for performing biliary interventions in liver transplant patients using the modified Hutson loop access (MHLA) and the impact of percutaneous endoscopy via the MHLA on these procedures.
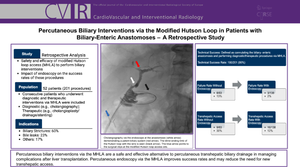
Methods: Over 13 years, 201 MHLA procedures were attempted on 52 patients (45 liver transplants; 24 living and 21 deceased donors) for diagnostic (e.g., cholangiography) and therapeutic (e.g., stent/drain insertion and cholangioplasty) purposes. The most common indications for MHLA were biliary strictures (60%) and bile leaks (23%). Percutaneous endoscopy was used to directly visualize the biliary-enteric anastomosis, diagnose pathology (e.g., ischemic cholangiopathy), and help in biliary hygiene (removing debris/casts/stones/stents) in 138/201 (69%) procedures. Technical success was defined as cannulating the biliary-enteric anastomosis and performing diagnostic/therapeutic procedure via the MHLA.
Results: The technical success rate was 95% (190/201). The failure rate among procedures performed with and without endoscopy was 2% (3/138) versus 13% (8/63) (P = 0.0024), and the need for new transhepatic access (to aid the procedure) was 12% (16/138) versus 30% (19/63) (P = 0.001). Despite endoscopy, failure in 2% of the cases resulted from inflamed/friable anastomosis (1/3) and high-grade stricture (2/3) obstructing retrograde cannulation of biliary-enteric anastomosis. Major adverse events (bowel perforation and injury) occurred in 1% of the procedures, with no procedure-related mortality.
Conclusions: MHLA-based percutaneous biliary intervention is a safe and effective alternative to managing complications after liver transplant. Percutaneous endoscopy via the MHLA improves success rates and may reduce the need for new transhepatic access. Level of Evidence Level 4.
期刊介绍:
CardioVascular and Interventional Radiology (CVIR) is the official journal of the Cardiovascular and Interventional Radiological Society of Europe, and is also the official organ of a number of additional distinguished national and international interventional radiological societies. CVIR publishes double blinded peer-reviewed original research work including clinical and laboratory investigations, technical notes, case reports, works in progress, and letters to the editor, as well as review articles, pictorial essays, editorials, and special invited submissions in the field of vascular and interventional radiology. Beside the communication of the latest research results in this field, it is also the aim of CVIR to support continuous medical education. Articles that are accepted for publication are done so with the understanding that they, or their substantive contents, have not been and will not be submitted to any other publication.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
