{"title":"Immunotherapy plus chemotherapy in patients with advanced endometrial cancer: a cost-effectiveness analysis.","authors":"Youwen Zhu, Kun Liu, Hong Zhu","doi":"10.3802/jgo.2025.36.e6","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Pembrolizumab and dostarlimab are immune checkpoint inhibitors that target programmed death receptor 1 (PD-1). Combination anti-PD-1 regimens have been shown to exhibit favorable survival benefits when treating advanced endometrial cancer (EC). Which treatment was preferable will need to be confirmed by a cost-effectiveness comparison between them.</p><p><strong>Methods: </strong>Based on patient and clinical parameters from RUBY and NRG-GY018 phase III randomized controlled trials, the Markov model with a 20-year time horizon was established to evaluate the cost-effectiveness of dostarlimab plus chemotherapy (DC), pembrolizumab plus chemotherapy (PC), and chemotherapy alone (C) treatment for patients with mismatch repair-proficient microsatellite-stable (pMMR-MSS) and mismatch repair-deficient microsatellite instability-high (dMMR-MSI-H) advanced EC from the American payers' perspective. The main results include total cost, life-years (LYs), quality-adjusted life-years (QALYs), and the incremental cost-effectiveness ratio (ICER) at a $150,000/QALY of willingness-to-pay.</p><p><strong>Results: </strong>In the pMMR-MSS population, DC, PC, and C produced costs (QALYs) of $99,205 (3.02), $322,530 (3.25), and $421,923 (4.40), resulting in corresponding ICERs of $974,177/QALY (PC vs. C), $234,527/QALY (DC vs. C), $86,671/QALY (DC vs. PC), respectively; In the dMMR-MSI-H population, DC, PC, and C obtained costs (QALYs) of $120,177 (5.73), $691,399 (8.43), and $708,787 (11.26), yielding ICERs of $266,423/QALY (PC vs. C), $135,165/QALY (DC vs. C), $7,866/QALY (DC vs. PC), respectively.</p><p><strong>Conclusion: </strong>In the US, DC was a more cost-effective treatment than PC for patients with advanced EC irrespective of MMR status. However, compared to C, DC was associated with more cost-effectiveness in the dMMR-MSI-H population.</p>","PeriodicalId":15868,"journal":{"name":"Journal of Gynecologic Oncology","volume":" ","pages":"e6"},"PeriodicalIF":3.7000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11790985/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Gynecologic Oncology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3802/jgo.2025.36.e6","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/3 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Pembrolizumab and dostarlimab are immune checkpoint inhibitors that target programmed death receptor 1 (PD-1). Combination anti-PD-1 regimens have been shown to exhibit favorable survival benefits when treating advanced endometrial cancer (EC). Which treatment was preferable will need to be confirmed by a cost-effectiveness comparison between them.
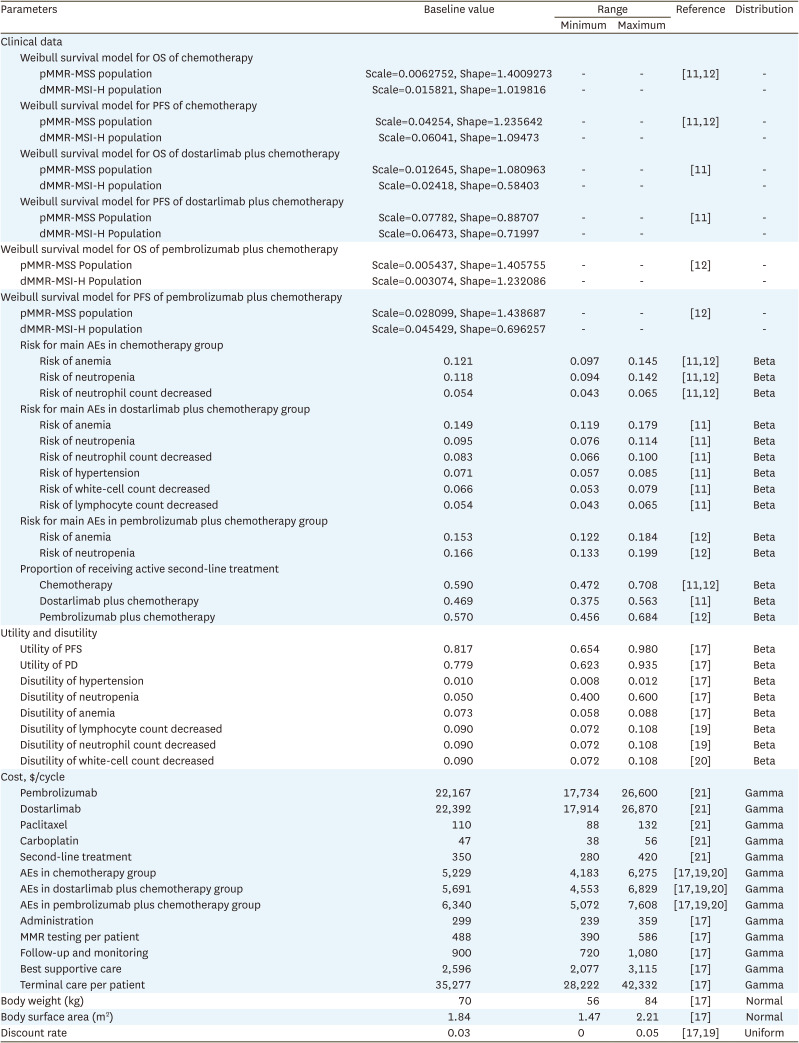
Methods: Based on patient and clinical parameters from RUBY and NRG-GY018 phase III randomized controlled trials, the Markov model with a 20-year time horizon was established to evaluate the cost-effectiveness of dostarlimab plus chemotherapy (DC), pembrolizumab plus chemotherapy (PC), and chemotherapy alone (C) treatment for patients with mismatch repair-proficient microsatellite-stable (pMMR-MSS) and mismatch repair-deficient microsatellite instability-high (dMMR-MSI-H) advanced EC from the American payers' perspective. The main results include total cost, life-years (LYs), quality-adjusted life-years (QALYs), and the incremental cost-effectiveness ratio (ICER) at a $150,000/QALY of willingness-to-pay.
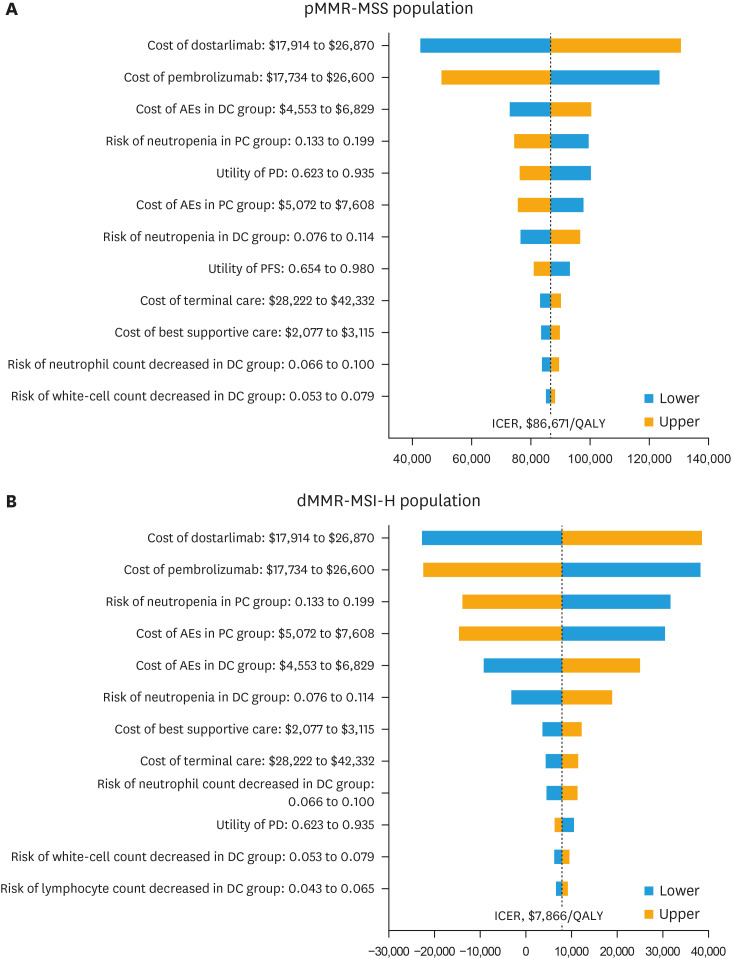
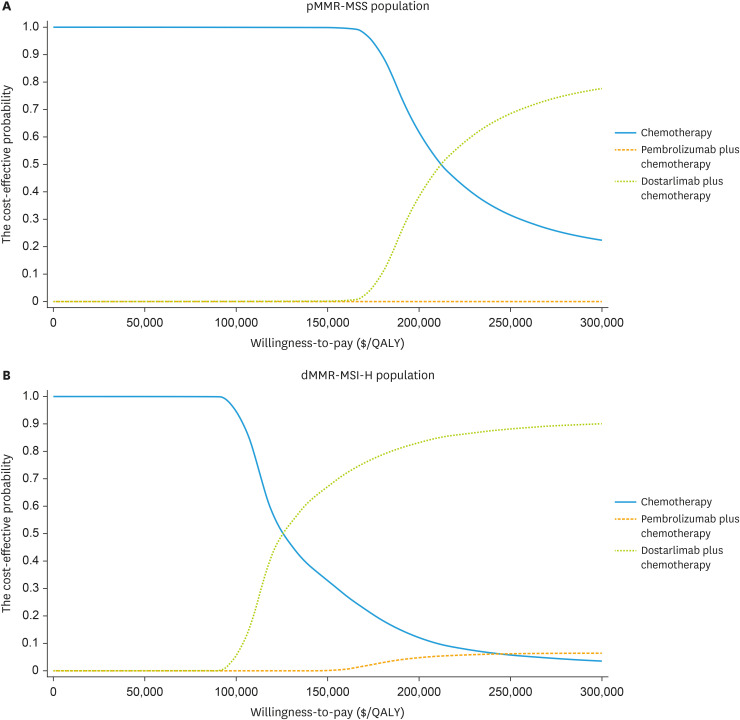
Results: In the pMMR-MSS population, DC, PC, and C produced costs (QALYs) of $99,205 (3.02), $322,530 (3.25), and $421,923 (4.40), resulting in corresponding ICERs of $974,177/QALY (PC vs. C), $234,527/QALY (DC vs. C), $86,671/QALY (DC vs. PC), respectively; In the dMMR-MSI-H population, DC, PC, and C obtained costs (QALYs) of $120,177 (5.73), $691,399 (8.43), and $708,787 (11.26), yielding ICERs of $266,423/QALY (PC vs. C), $135,165/QALY (DC vs. C), $7,866/QALY (DC vs. PC), respectively.
Conclusion: In the US, DC was a more cost-effective treatment than PC for patients with advanced EC irrespective of MMR status. However, compared to C, DC was associated with more cost-effectiveness in the dMMR-MSI-H population.
期刊介绍:
The Journal of Gynecologic Oncology (JGO) is an official publication of the Asian Society of Gynecologic Oncology. Abbreviated title is ''J Gynecol Oncol''. It was launched in 1990. The JGO''s aim is to publish the highest quality manuscripts dedicated to the advancement of care of the patients with gynecologic cancer. It is an international peer-reviewed periodical journal that is published bimonthly (January, March, May, July, September, and November). Supplement numbers are at times published. The journal publishes editorials, original and review articles, correspondence, book review, etc.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
