{"title":"Intensity of statin therapy after ischaemic stroke and long-term outcomes: a nationwide cohort study.","authors":"Ville Kytö, Julia Åivo, Jori O Ruuskanen","doi":"10.1136/svn-2024-003230","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Statins are essential for secondary prevention after ischaemic stroke (IS). However, statin intensity recommendations differ, and there is a concern about intracerebral haemorrhage (ICH). We studied the long-term impacts of initial statin intensity following IS.</p><p><strong>Methods: </strong>Consecutive patients using high-intensity, moderate-intensity or low-intensity statin early after IS (n=45 512) were retrospectively studied using national registries in Finland. Differences were adjusted using multivariable regression. The primary outcome was all-cause death within 12-year follow-up (median 5.9 years). Secondary outcomes were recurrent IS, cardiovascular death and ICH studied using competing risk analyses.</p><p><strong>Results: </strong>High-intensity therapy was initially used by 16.0%, moderate-intensity by 73.8% and low-intensity by 10.2%. Risk of death was lower with high-intensity versus moderate-intensity (adjusted HR (adj.HR) 0.92; 95% CI 0.87 to 0.97; number needed to treat (NNT) 32.0), with moderate-intensity versus low-intensity (adj.HR 0.91; 95% CI 0.87 to 0.95; NNT 27.5) and with high-intensity versus low-intensity (adj.HR 0.83; 95% CI 0.78 to 0.89; NNT 14.6) statin. There was a dose-dependent association of initial statin intensity with a lower probability of recurrent IS (p<0.0001) and cardiovascular death (p<0.0001). The occurrence of ICH was not associated with initial statin intensity (p=0.646).</p><p><strong>Conclusions: </strong>Following IS, more intense initial statin treatment is associated with improved long-term outcomes but not with the risk of ICH. These findings emphasise the importance of high statin intensity shortly after IS.</p>","PeriodicalId":48733,"journal":{"name":"Journal of Investigative Medicine","volume":" ","pages":"142-145"},"PeriodicalIF":4.9000,"publicationDate":"2025-02-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11877428/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Investigative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/svn-2024-003230","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Statins are essential for secondary prevention after ischaemic stroke (IS). However, statin intensity recommendations differ, and there is a concern about intracerebral haemorrhage (ICH). We studied the long-term impacts of initial statin intensity following IS.
Methods: Consecutive patients using high-intensity, moderate-intensity or low-intensity statin early after IS (n=45 512) were retrospectively studied using national registries in Finland. Differences were adjusted using multivariable regression. The primary outcome was all-cause death within 12-year follow-up (median 5.9 years). Secondary outcomes were recurrent IS, cardiovascular death and ICH studied using competing risk analyses.
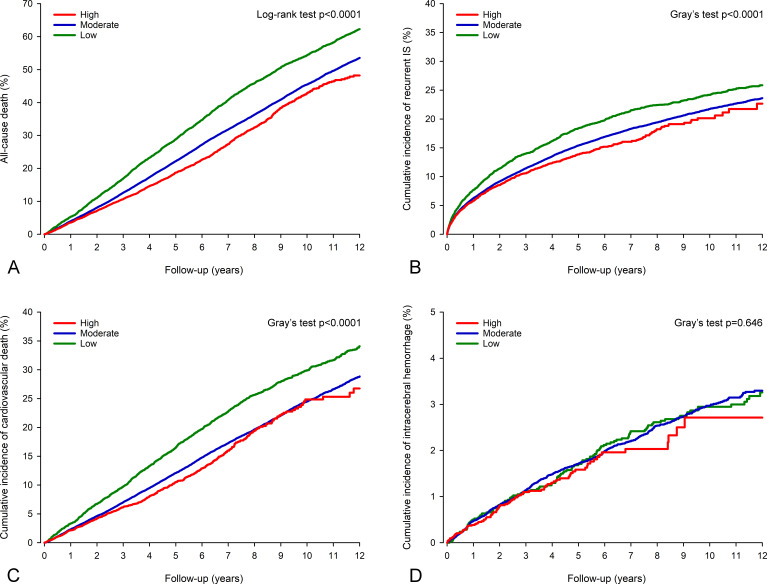
Results: High-intensity therapy was initially used by 16.0%, moderate-intensity by 73.8% and low-intensity by 10.2%. Risk of death was lower with high-intensity versus moderate-intensity (adjusted HR (adj.HR) 0.92; 95% CI 0.87 to 0.97; number needed to treat (NNT) 32.0), with moderate-intensity versus low-intensity (adj.HR 0.91; 95% CI 0.87 to 0.95; NNT 27.5) and with high-intensity versus low-intensity (adj.HR 0.83; 95% CI 0.78 to 0.89; NNT 14.6) statin. There was a dose-dependent association of initial statin intensity with a lower probability of recurrent IS (p<0.0001) and cardiovascular death (p<0.0001). The occurrence of ICH was not associated with initial statin intensity (p=0.646).
Conclusions: Following IS, more intense initial statin treatment is associated with improved long-term outcomes but not with the risk of ICH. These findings emphasise the importance of high statin intensity shortly after IS.
背景:他汀类药物是缺血性卒中(IS)二级预防的基本药物。然而,他汀类药物的强度建议各不相同,而且人们对脑内出血(ICH)也存在担忧。我们研究了 IS 后初始他汀类药物强度的长期影响:方法:我们利用芬兰国家登记册对IS后早期使用高强度、中等强度或低强度他汀的连续患者(n=45 512)进行了回顾性研究。采用多变量回归对差异进行了调整。主要结果是随访 12 年(中位数 5.9 年)内的全因死亡。次要结果是复发性IS、心血管死亡和ICH,采用竞争风险分析进行研究:16.0%的患者最初使用了高强度治疗,73.8%的患者使用了中强度治疗,10.2%的患者使用了低强度治疗。使用高强度他汀与中强度他汀相比(调整HR(adj.HR)0.92;95% CI 0.87至0.97;治疗需要量(NNT)32.0),中强度他汀与低强度他汀相比(adj.HR 0.91;95% CI 0.87至0.95;NNT 27.5),以及高强度他汀与低强度他汀相比(adj.HR 0.83;95% CI 0.78至0.89;NNT 14.6),死亡风险均较低。初始他汀强度与较低的IS复发概率存在剂量依赖关系(p结论:IS发生后,初始他汀类药物治疗强度越高,长期预后越好,但发生ICH的风险却不高。这些发现强调了IS发生后短期内高强度他汀类药物治疗的重要性。
期刊介绍:
Journal of Investigative Medicine (JIM) is the official publication of the American Federation for Medical Research. The journal is peer-reviewed and publishes high-quality original articles and reviews in the areas of basic, clinical, and translational medical research.
JIM publishes on all topics and specialty areas that are critical to the conduct of the entire spectrum of biomedical research: from the translation of clinical observations at the bedside, to basic and animal research to clinical research and the implementation of innovative medical care.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
