Signal intensity and volume of carotid intraplaque hemorrhage on magnetic resonance imaging and the risk of ipsilateral cerebrovascular events: The Plaque At RISK (PARISK) study.
Kelly P H Nies, Mueez Aizaz, Dianne H K van Dam-Nolen, Timothy C D Goring, Tobien A H C M L Schreuder, Narender P van Orshoven, Alida A Postma, Daniel Bos, Jeroen Hendrikse, Paul Nederkoorn, Rob van der Geest, Robert J van Oostenbrugge, Werner H Mess, M Eline Kooi
{"title":"Signal intensity and volume of carotid intraplaque hemorrhage on magnetic resonance imaging and the risk of ipsilateral cerebrovascular events: The Plaque At RISK (PARISK) study.","authors":"Kelly P H Nies, Mueez Aizaz, Dianne H K van Dam-Nolen, Timothy C D Goring, Tobien A H C M L Schreuder, Narender P van Orshoven, Alida A Postma, Daniel Bos, Jeroen Hendrikse, Paul Nederkoorn, Rob van der Geest, Robert J van Oostenbrugge, Werner H Mess, M Eline Kooi","doi":"10.1016/j.jocmr.2024.101049","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Plaque At RISK (PARISK) study demonstrated that patients with a carotid plaque with intraplaque hemorrhage (IPH) have an increased risk of recurrent ipsilateral ischemic cerebrovascular events. It was previously reported that symptomatic carotid plaques with IPH showed higher IPH signal intensity ratios (SIR) and larger IPH volumes than asymptomatic plaques. We explored whether IPH SIR and IPH volume are associated with future ipsilateral ischemic cerebrovascular events beyond the presence of IPH.</p><p><strong>Methods: </strong>Transient ischemic attack and ischemic stroke patients with mild-to-moderate carotid stenosis and an ipsilateral IPH-positive carotid plaque (n = 89) from the PARISK study were included. The clinical endpoint was a new ipsilateral ischemic cerebrovascular event during 5 years of follow-up, while the imaging-based endpoint was a new ipsilateral brain infarct on brain magnetic resonance imaging (MRI) after 2 years (n = 69). Trained observers delineated IPH, a hyperintense region compared to surrounding muscle tissue on hyper T<sub>1</sub>-weighted magnetic resonance images. The IPH SIR was the maximal signal intensity in the IPH region divided by the mean signal intensity of adjacent muscle tissue. The associations between IPH SIR or volume and the clinical and imaging-based endpoint were investigated using Cox proportional hazard models and logistic regression, respectively.</p><p><strong>Results: </strong>During 5.1 (interquartile range: 3.1-5.6) years of follow-up, 21 ipsilateral cerebrovascular ischemic events were identified. Twelve new ipsilateral brain infarcts were identified on the 2-year neuro MRI. There was no association for IPH SIR or IPH volume with the clinical endpoint (hazard ratio (HR): 0.89 [95% confidence interval: 0.67-1.10] and HR: 0.91 [0.69-1.19] per 100-µL increase, respectively) nor with the imaging-based endpoint (odds ratio (OR): 1.04 [0.75-1.45] and OR: 1.21 [0.87-1.68] per 100-µL increase, respectively).</p><p><strong>Conclusion: </strong>IPH SIR and IPH volume were not associated with future ipsilateral ischemic cerebrovascular events. Therefore, quantitative assessment of IPH of SIR and volume does not seem to provide additional value beyond the presence of IPH for stroke risk assessment.</p><p><strong>Trial registration: </strong>The PARISK study was registered on ClinicalTrials.gov with ID NCT01208025 on September 21, 2010 (https://clinicaltrials.gov/study/NCT01208025).</p>","PeriodicalId":15221,"journal":{"name":"Journal of Cardiovascular Magnetic Resonance","volume":" ","pages":"101049"},"PeriodicalIF":6.1000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11282977/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Magnetic Resonance","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.jocmr.2024.101049","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/13 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
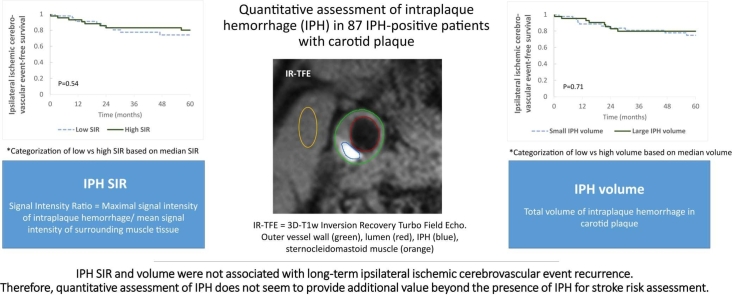
Background: The Plaque At RISK (PARISK) study demonstrated that patients with a carotid plaque with intraplaque hemorrhage (IPH) have an increased risk of recurrent ipsilateral ischemic cerebrovascular events. It was previously reported that symptomatic carotid plaques with IPH showed higher IPH signal intensity ratios (SIR) and larger IPH volumes than asymptomatic plaques. We explored whether IPH SIR and IPH volume are associated with future ipsilateral ischemic cerebrovascular events beyond the presence of IPH.
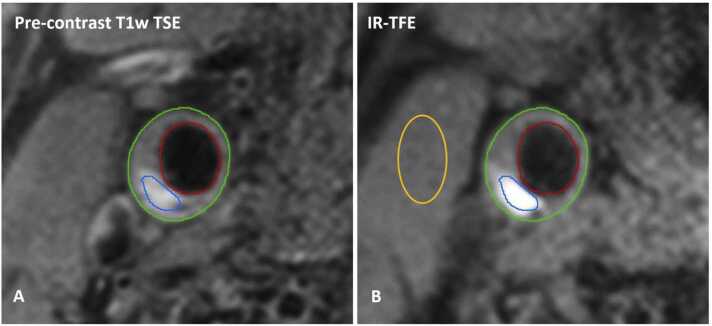
Methods: Transient ischemic attack and ischemic stroke patients with mild-to-moderate carotid stenosis and an ipsilateral IPH-positive carotid plaque (n = 89) from the PARISK study were included. The clinical endpoint was a new ipsilateral ischemic cerebrovascular event during 5 years of follow-up, while the imaging-based endpoint was a new ipsilateral brain infarct on brain magnetic resonance imaging (MRI) after 2 years (n = 69). Trained observers delineated IPH, a hyperintense region compared to surrounding muscle tissue on hyper T1-weighted magnetic resonance images. The IPH SIR was the maximal signal intensity in the IPH region divided by the mean signal intensity of adjacent muscle tissue. The associations between IPH SIR or volume and the clinical and imaging-based endpoint were investigated using Cox proportional hazard models and logistic regression, respectively.
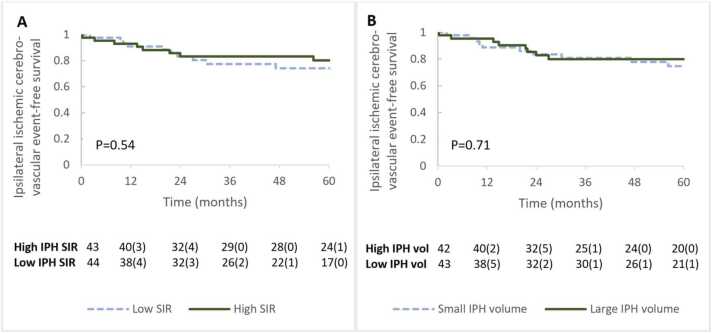
Results: During 5.1 (interquartile range: 3.1-5.6) years of follow-up, 21 ipsilateral cerebrovascular ischemic events were identified. Twelve new ipsilateral brain infarcts were identified on the 2-year neuro MRI. There was no association for IPH SIR or IPH volume with the clinical endpoint (hazard ratio (HR): 0.89 [95% confidence interval: 0.67-1.10] and HR: 0.91 [0.69-1.19] per 100-µL increase, respectively) nor with the imaging-based endpoint (odds ratio (OR): 1.04 [0.75-1.45] and OR: 1.21 [0.87-1.68] per 100-µL increase, respectively).
Conclusion: IPH SIR and IPH volume were not associated with future ipsilateral ischemic cerebrovascular events. Therefore, quantitative assessment of IPH of SIR and volume does not seem to provide additional value beyond the presence of IPH for stroke risk assessment.
Trial registration: The PARISK study was registered on ClinicalTrials.gov with ID NCT01208025 on September 21, 2010 (https://clinicaltrials.gov/study/NCT01208025).
期刊介绍:
Journal of Cardiovascular Magnetic Resonance (JCMR) publishes high-quality articles on all aspects of basic, translational and clinical research on the design, development, manufacture, and evaluation of cardiovascular magnetic resonance (CMR) methods applied to the cardiovascular system. Topical areas include, but are not limited to:
New applications of magnetic resonance to improve the diagnostic strategies, risk stratification, characterization and management of diseases affecting the cardiovascular system.
New methods to enhance or accelerate image acquisition and data analysis.
Results of multicenter, or larger single-center studies that provide insight into the utility of CMR.
Basic biological perceptions derived by CMR methods.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
