Sahar J. Farahani, Joshua Li, Beatrice Minder, Philippe Vielh, Marija Glisic, Taulant Muka
{"title":"Impact of implementing the first edition of the Paris system for reporting: A systematic review and meta-analysis","authors":"Sahar J. Farahani, Joshua Li, Beatrice Minder, Philippe Vielh, Marija Glisic, Taulant Muka","doi":"10.1111/cyt.13407","DOIUrl":null,"url":null,"abstract":"<p>Urine cytology is a noninvasive, widely used diagnostic tool for screening and surveillance of genitourinary tract neoplasms. However, the absence of unified terminology and clear objective morphological criteria limits the clinical benefit of urine cytology. The Paris System for Reporting Urine Cytology (TPS) was developed with the goal of standardizing reporting and improving urine cytology performance in detecting high-grade malignancy (HGM). We aimed to evaluate potential effects of TPS on improving urine cytology diagnostic performance and clinical utility by conducting a systematic review and meta-analysis. We searched six electronic databases to identify cross-sectional and cohort studies written in English assessing the accuracy of urine cytology in detecting genitourinary tract malignancies of patients under surveillance or with clinical suspicion of malignancy from January 2004 to December 2022. We extracted relevant data from eligible studies to calculate relative distribution of cytology diagnostic categories; ratio of atypical to HGM cytology diagnosis; and risk of HGM (ROHGM) and HGM likelihood ratio (HGM-LR) associated with cytology diagnostic categories. We used a generalized linear mixed model with logit transformation to combine proportions and multilevel mixed-effect logistic regression to pool diagnostic accuracy measurements. We performed meta-regression to evaluate any significant difference between TPS and non-TPS cohorts. We included 64 studies for 99,796 combined total cytology samples, across 31 TPS and 49 non-TPS cohorts. Pooled relative distribution [95% confidence interval (CI)] of negative for high-grade urothelial carcinoma (NHGUC)/negative for malignancy (NM); atypical urothelial cells (AUC); suspicious for high-grade urothelial carcinoma (SHGUC)/suspicious for malignancy (SM); low-grade urothelial neoplasm (LGUN); and HGM categories among satisfactory cytology cases were 83.8% (80.3%–86.9%), 8.0% (6.0%–10.6%), 2.2% (1.4%–3.3%), 0.01% (0.0%–0.1%), and 4.2% (3.2%–5.5%) in TPS versus 80.8% (76.8–2.7%), 11.3% (8.6%–14.7%), 1.8% (1.2%–2.7%), 0.01% (0.0%–0.1%), and 3.3% (2.5%–4.3%) in non-TPS cohorts. Adopting TPS classification resulted in a significant increase in the frequency of NHGUC and a reduction in AUC cytology diagnoses, respectively. The AUC/HGM ratio in TPS cohort was 2.0, which showed a statistically significant difference from the atypical/HGM ratio of 4.1 in non-TPS cohort (<i>p</i>-value: 0.01). Moreover, the summary rate (95% CI) of LGUN called AUC on cytology significantly decreased to 20.8% (14.9%–28.3%) in the TPS compared with 34.1% (26.4%–42.8%) in non-TPS cohorts. The pooled ROHGM (95% CI) was 20.4% (6.2%–50.0%) in nondiagnostic (NDX), 15.5% (9.6%–24.2%) in NHGUC, 40.2% (30.9%–50.2%) in AUC, 80.8% (72.9%–86.8%) in SHGUC, 15.1% (5.7%–34.3%) in LGUN, and 91.4% (87.3%–94.3%) in HGM categories in TPS studies. NHGUC, AUC, SHGUC, and HGM categories were associated with HGM-LR (95% CI) of 0.2 (0.1–0.3), 0.9 (0.6–1.3), 6.9 (2.4–19.9), and 16.8 (8.3–33.8). Our results suggest that TPS 1.0 has reduced the relative frequency of AUC diagnosis, AUC/HGM ratio, and the frequency of LGUNs diagnosed as AUC on cytology. Adopting this classification has improved the clinical utility of SHGUC and HGM cytology diagnoses in ruling in high-grade lesions. However, an NHGUC diagnosis does not reliably rule out the presence of a high-grade lesion.</p>","PeriodicalId":55187,"journal":{"name":"Cytopathology","volume":"35 5","pages":"616-633"},"PeriodicalIF":1.1000,"publicationDate":"2024-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cytopathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/cyt.13407","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"CELL BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
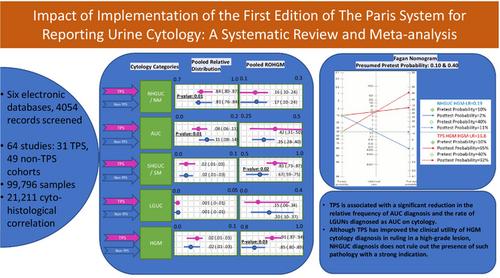
Urine cytology is a noninvasive, widely used diagnostic tool for screening and surveillance of genitourinary tract neoplasms. However, the absence of unified terminology and clear objective morphological criteria limits the clinical benefit of urine cytology. The Paris System for Reporting Urine Cytology (TPS) was developed with the goal of standardizing reporting and improving urine cytology performance in detecting high-grade malignancy (HGM). We aimed to evaluate potential effects of TPS on improving urine cytology diagnostic performance and clinical utility by conducting a systematic review and meta-analysis. We searched six electronic databases to identify cross-sectional and cohort studies written in English assessing the accuracy of urine cytology in detecting genitourinary tract malignancies of patients under surveillance or with clinical suspicion of malignancy from January 2004 to December 2022. We extracted relevant data from eligible studies to calculate relative distribution of cytology diagnostic categories; ratio of atypical to HGM cytology diagnosis; and risk of HGM (ROHGM) and HGM likelihood ratio (HGM-LR) associated with cytology diagnostic categories. We used a generalized linear mixed model with logit transformation to combine proportions and multilevel mixed-effect logistic regression to pool diagnostic accuracy measurements. We performed meta-regression to evaluate any significant difference between TPS and non-TPS cohorts. We included 64 studies for 99,796 combined total cytology samples, across 31 TPS and 49 non-TPS cohorts. Pooled relative distribution [95% confidence interval (CI)] of negative for high-grade urothelial carcinoma (NHGUC)/negative for malignancy (NM); atypical urothelial cells (AUC); suspicious for high-grade urothelial carcinoma (SHGUC)/suspicious for malignancy (SM); low-grade urothelial neoplasm (LGUN); and HGM categories among satisfactory cytology cases were 83.8% (80.3%–86.9%), 8.0% (6.0%–10.6%), 2.2% (1.4%–3.3%), 0.01% (0.0%–0.1%), and 4.2% (3.2%–5.5%) in TPS versus 80.8% (76.8–2.7%), 11.3% (8.6%–14.7%), 1.8% (1.2%–2.7%), 0.01% (0.0%–0.1%), and 3.3% (2.5%–4.3%) in non-TPS cohorts. Adopting TPS classification resulted in a significant increase in the frequency of NHGUC and a reduction in AUC cytology diagnoses, respectively. The AUC/HGM ratio in TPS cohort was 2.0, which showed a statistically significant difference from the atypical/HGM ratio of 4.1 in non-TPS cohort (p-value: 0.01). Moreover, the summary rate (95% CI) of LGUN called AUC on cytology significantly decreased to 20.8% (14.9%–28.3%) in the TPS compared with 34.1% (26.4%–42.8%) in non-TPS cohorts. The pooled ROHGM (95% CI) was 20.4% (6.2%–50.0%) in nondiagnostic (NDX), 15.5% (9.6%–24.2%) in NHGUC, 40.2% (30.9%–50.2%) in AUC, 80.8% (72.9%–86.8%) in SHGUC, 15.1% (5.7%–34.3%) in LGUN, and 91.4% (87.3%–94.3%) in HGM categories in TPS studies. NHGUC, AUC, SHGUC, and HGM categories were associated with HGM-LR (95% CI) of 0.2 (0.1–0.3), 0.9 (0.6–1.3), 6.9 (2.4–19.9), and 16.8 (8.3–33.8). Our results suggest that TPS 1.0 has reduced the relative frequency of AUC diagnosis, AUC/HGM ratio, and the frequency of LGUNs diagnosed as AUC on cytology. Adopting this classification has improved the clinical utility of SHGUC and HGM cytology diagnoses in ruling in high-grade lesions. However, an NHGUC diagnosis does not reliably rule out the presence of a high-grade lesion.
期刊介绍:
The aim of Cytopathology is to publish articles relating to those aspects of cytology which will increase our knowledge and understanding of the aetiology, diagnosis and management of human disease. It contains original articles and critical reviews on all aspects of clinical cytology in its broadest sense, including: gynaecological and non-gynaecological cytology; fine needle aspiration and screening strategy.
Cytopathology welcomes papers and articles on: ultrastructural, histochemical and immunocytochemical studies of the cell; quantitative cytology and DNA hybridization as applied to cytological material.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
