Tove Tveitan Borgen, Sindre Lee-Ødegård, Barbara Fink Eriksen, Erik Fink Eriksen
{"title":"Intermittent dosing of zoledronic acid based on bone turnover marker assessment reduces vertebral and non-vertebral fractures.","authors":"Tove Tveitan Borgen, Sindre Lee-Ødegård, Barbara Fink Eriksen, Erik Fink Eriksen","doi":"10.1093/jbmrpl/ziae072","DOIUrl":null,"url":null,"abstract":"<p><p>Previous studies have demonstrated that the administration of zoledronic acid (ZOL) once yearly for 3 years or once over 3 years, yields similar antifracture efficacy. Bone turnover markers can predict the antifracture efficacy of antiresorptive agents, with procollagen type 1 N-terminal propeptide (P1NP) being the most useful marker. In this retrospective cohort study, we explored the effects of intravenous dosing of ZOL guided by serum (S)-P1NP assessment on bone mineral density (BMD) and fractures. Consenting patients (<i>N</i> = 202, mean age 68.2 years) with osteoporosis were treated with ZOL for an average of 4.4 (range 2-8) years. S-P1NP and BMD were measured at baseline and every 1-2 years. We assessed the number of subsequent vertebral and nonvertebral fractures in the 2-year time periods. The number of patients assessed was 202, 147, 69, and 29 at years 1-2, 3-4, 5-6, and 7-8, respectively. A new ZOL infusion was given if S-P1NP exhibited values above 35 μg/L. BMD increased by 6.2% (SD 4.0) over the first 2 years and stabilized in years 2-8 (<i>P</i> <.05). Median S-P1NP exhibited an initial reduction from 58.0 to 31.3 μg/L at year 2 and then increased to 39.0 μg/L at years 7-8. Compared with fractures observed in the last 2 years before baseline, fracture rates exhibited consistent reductions, for vertebral fractures odds ratio (OR) [95% confidence interval] = 0.61 [0.47, 0.80], <i>P</i> <.001 and for nonvertebral fractures OR = 0.23 [0.18, 0.31], <i>P</i> <.001. In conclusion, intermittent dosing of intravenous ZOL based on the assessment of S-P1NP with cut-off at 35 μg/L resulted in an initial increase followed by a stable BMD, suppression of S-P1NP, and stable reduction of fractures for 8 years. Only 39% of patients needed more than one infusion. This approach reduces healthcare costs and might also reduce the risk of rare side effects such as osteonecrosis of the jaw and atypical femoral fracture.</p>","PeriodicalId":14611,"journal":{"name":"JBMR Plus","volume":"8 7","pages":"ziae072"},"PeriodicalIF":2.4000,"publicationDate":"2024-05-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11208720/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JBMR Plus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/jbmrpl/ziae072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
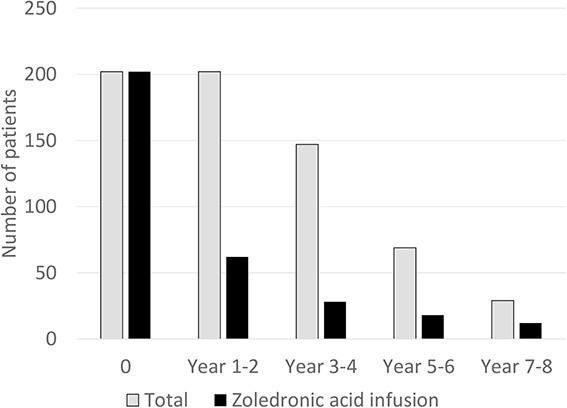
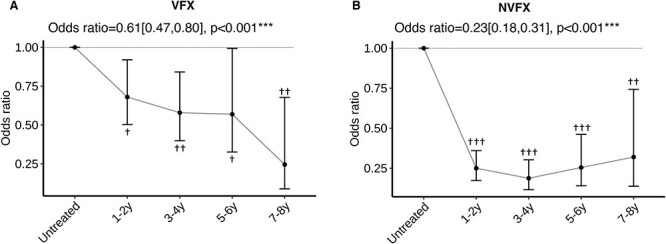
Previous studies have demonstrated that the administration of zoledronic acid (ZOL) once yearly for 3 years or once over 3 years, yields similar antifracture efficacy. Bone turnover markers can predict the antifracture efficacy of antiresorptive agents, with procollagen type 1 N-terminal propeptide (P1NP) being the most useful marker. In this retrospective cohort study, we explored the effects of intravenous dosing of ZOL guided by serum (S)-P1NP assessment on bone mineral density (BMD) and fractures. Consenting patients (N = 202, mean age 68.2 years) with osteoporosis were treated with ZOL for an average of 4.4 (range 2-8) years. S-P1NP and BMD were measured at baseline and every 1-2 years. We assessed the number of subsequent vertebral and nonvertebral fractures in the 2-year time periods. The number of patients assessed was 202, 147, 69, and 29 at years 1-2, 3-4, 5-6, and 7-8, respectively. A new ZOL infusion was given if S-P1NP exhibited values above 35 μg/L. BMD increased by 6.2% (SD 4.0) over the first 2 years and stabilized in years 2-8 (P <.05). Median S-P1NP exhibited an initial reduction from 58.0 to 31.3 μg/L at year 2 and then increased to 39.0 μg/L at years 7-8. Compared with fractures observed in the last 2 years before baseline, fracture rates exhibited consistent reductions, for vertebral fractures odds ratio (OR) [95% confidence interval] = 0.61 [0.47, 0.80], P <.001 and for nonvertebral fractures OR = 0.23 [0.18, 0.31], P <.001. In conclusion, intermittent dosing of intravenous ZOL based on the assessment of S-P1NP with cut-off at 35 μg/L resulted in an initial increase followed by a stable BMD, suppression of S-P1NP, and stable reduction of fractures for 8 years. Only 39% of patients needed more than one infusion. This approach reduces healthcare costs and might also reduce the risk of rare side effects such as osteonecrosis of the jaw and atypical femoral fracture.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
