{"title":"Long-Term Differential Effects of Gastric Bypass and Sleeve Gastrectomy on Bone Mineral Density.","authors":"Pierre-Emmanuel Cailleaux, Agnès Ostertag, Didier Albert Haguenauer, Séverine Ledoux, Martine Cohen-Solal","doi":"10.1210/jendso/bvae111","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>The association of obesity with bone fragility fractures is complex and non-linear. Despite good efficacy on weight loss, bariatric surgery (BS) is also associated with bone loss. However, we lack information on risk factors of the long-term deleterious effects of BS on the skeleton.</p><p><strong>Objective: </strong>We aimed to assess the factors associated with low bone mineral density (BMD) performed a long time after Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG).</p><p><strong>Methods: </strong>This cross-sectional study involved patients at a long distance from their BS that underwent dual-energy x-ray absorptiometry (DXA) with biological factors (vitamins, micronutrients, bone and inflammation biomarkers). Simple and multiple linear models (stepwise and parsimony approach) were developed.</p><p><strong>Results: </strong>A total of 131 patients (91 RYGB, 40 SG) underwent DXA (51.8 ± 11.08 years, 87.8% women). At a mean of 6.8 ± 3.7 years after surgery, the mean weight loss was -28.6 ± 9.6%, and only 6 patients (5.7%) had a <i>T</i>-score less than or equal to -2.5. On univariate analysis, BMD was lower in the RYGB than in the SG group (<i>P</i> < .001) at all sites, despite similar fat and fat-free mass and weight loss. Serum parathyroid hormone and phosphate levels were higher in RYGB than SG patients. A total of 10.1% of patients showed vascular calcifications. On multivariable analysis, BMD remained different between surgery groups after adjustment for age, body mass index, ethnicity, and sex. The model-adjusted <i>R</i> <sup>2</sup> values were 0.451 for the total hip; 0.462 the femoral neck, and 0.191 the lumbar spine for the inflammation model; 0.458, 0.462, and 0.254, respectively, for the bone marker model; and 0.372, 0.396, and 0.142 for the vitamin model. Serum zinc, ferritin, and uric acid levels were the markers associated with BMD to a low extent.</p><p><strong>Conclusion: </strong>BMD differed depending on the BS procedure. A few biological markers may be associated weakly with BMD well after the surgery.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"8 7","pages":"bvae111"},"PeriodicalIF":3.1000,"publicationDate":"2024-06-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11210305/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvae111","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/23 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Context: The association of obesity with bone fragility fractures is complex and non-linear. Despite good efficacy on weight loss, bariatric surgery (BS) is also associated with bone loss. However, we lack information on risk factors of the long-term deleterious effects of BS on the skeleton.
Objective: We aimed to assess the factors associated with low bone mineral density (BMD) performed a long time after Roux-en-Y gastric bypass (RYGB) or sleeve gastrectomy (SG).
Methods: This cross-sectional study involved patients at a long distance from their BS that underwent dual-energy x-ray absorptiometry (DXA) with biological factors (vitamins, micronutrients, bone and inflammation biomarkers). Simple and multiple linear models (stepwise and parsimony approach) were developed.
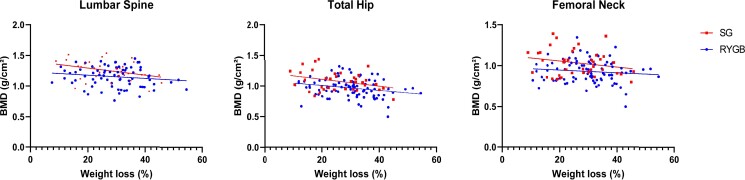
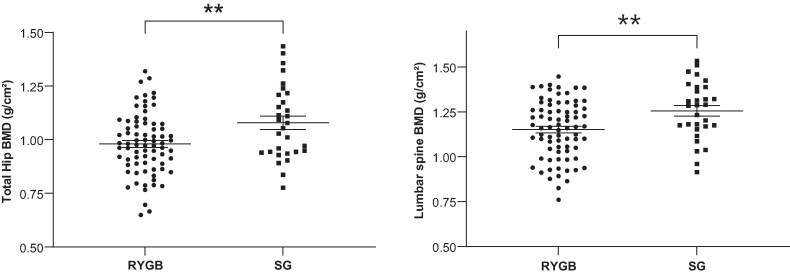
Results: A total of 131 patients (91 RYGB, 40 SG) underwent DXA (51.8 ± 11.08 years, 87.8% women). At a mean of 6.8 ± 3.7 years after surgery, the mean weight loss was -28.6 ± 9.6%, and only 6 patients (5.7%) had a T-score less than or equal to -2.5. On univariate analysis, BMD was lower in the RYGB than in the SG group (P < .001) at all sites, despite similar fat and fat-free mass and weight loss. Serum parathyroid hormone and phosphate levels were higher in RYGB than SG patients. A total of 10.1% of patients showed vascular calcifications. On multivariable analysis, BMD remained different between surgery groups after adjustment for age, body mass index, ethnicity, and sex. The model-adjusted R2 values were 0.451 for the total hip; 0.462 the femoral neck, and 0.191 the lumbar spine for the inflammation model; 0.458, 0.462, and 0.254, respectively, for the bone marker model; and 0.372, 0.396, and 0.142 for the vitamin model. Serum zinc, ferritin, and uric acid levels were the markers associated with BMD to a low extent.
Conclusion: BMD differed depending on the BS procedure. A few biological markers may be associated weakly with BMD well after the surgery.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
