{"title":"Bilothorax: A Case Report and Systematic Literature Review of the Rare Entity.","authors":"Roshan Acharya, Smita Kafle, Yub Raj Sedhai, Dhan Bahadur Shrestha, Kevin Walsh, Wasif Elahi Shamsi, Suraj Gyawali, Nikita Acharya, Anthony Lukas Loschner, Edmundo Raul Rubio","doi":"10.1155/2024/3973056","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bilothorax is defined as the presence of bile in the pleural space. It is a rare condition, and diagnosis is confirmed with a pleural fluid-to-serum bilirubin ratio of >1.</p><p><strong>Methods: </strong>The PubMed, Embase, Google Scholar, and CINAHL databases were searched using predetermined Boolean parameters. The systematic literature review was done per PRISMA guidelines. Retrospective studies, case series, case reports, and conference abstracts were included. The patients with reported pleural fluid analyses were pooled for fluid parameter data analysis.</p><p><strong>Results: </strong>Of 838 articles identified through the inclusion criteria and removing 105 duplicates, 732 articles were screened with abstracts, and 285 were screened for full article review. After this, 123 studies qualified for further detailed review, and of these, 115 were pooled for data analysis. The mean pleural fluid and serum bilirubin levels were 72 mg/dL and 61 mg/dL, respectively, with a mean pleural fluid-to-serum bilirubin ratio of 3.47. In most cases, the bilothorax was reported as a subacute or remote complication of hepatobiliary surgery or procedure, and traumatic injury to the chest or abdomen was the second most common cause. Tube thoracostomy was the main treatment modality (73.83%), followed by serial thoracentesis. Fifty-two patients (51.30%) had associated bronchopleural fistulas. The mortality was considerable, with 18/115 (15.65%) reported death. Most of the patients with mortality had advanced hepatobiliary cancer and were noted to die of complications not related to bilothorax.</p><p><strong>Conclusion: </strong>Bilothorax should be suspected in patients presenting with pleural effusion following surgical manipulation of hepatobiliary structures or a traumatic injury to the chest. This review is registered with CRD42023438426.</p>","PeriodicalId":46434,"journal":{"name":"Pulmonary Medicine","volume":"2024 ","pages":"3973056"},"PeriodicalIF":2.1000,"publicationDate":"2024-06-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11213635/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pulmonary Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2024/3973056","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Bilothorax is defined as the presence of bile in the pleural space. It is a rare condition, and diagnosis is confirmed with a pleural fluid-to-serum bilirubin ratio of >1.
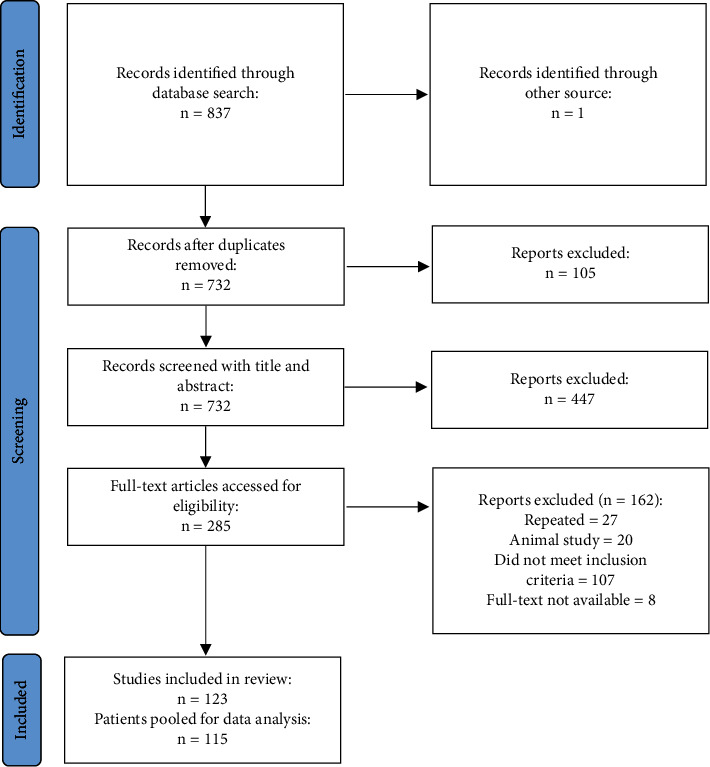
Methods: The PubMed, Embase, Google Scholar, and CINAHL databases were searched using predetermined Boolean parameters. The systematic literature review was done per PRISMA guidelines. Retrospective studies, case series, case reports, and conference abstracts were included. The patients with reported pleural fluid analyses were pooled for fluid parameter data analysis.
Results: Of 838 articles identified through the inclusion criteria and removing 105 duplicates, 732 articles were screened with abstracts, and 285 were screened for full article review. After this, 123 studies qualified for further detailed review, and of these, 115 were pooled for data analysis. The mean pleural fluid and serum bilirubin levels were 72 mg/dL and 61 mg/dL, respectively, with a mean pleural fluid-to-serum bilirubin ratio of 3.47. In most cases, the bilothorax was reported as a subacute or remote complication of hepatobiliary surgery or procedure, and traumatic injury to the chest or abdomen was the second most common cause. Tube thoracostomy was the main treatment modality (73.83%), followed by serial thoracentesis. Fifty-two patients (51.30%) had associated bronchopleural fistulas. The mortality was considerable, with 18/115 (15.65%) reported death. Most of the patients with mortality had advanced hepatobiliary cancer and were noted to die of complications not related to bilothorax.
Conclusion: Bilothorax should be suspected in patients presenting with pleural effusion following surgical manipulation of hepatobiliary structures or a traumatic injury to the chest. This review is registered with CRD42023438426.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
