O A Badejo, E C Nwafuluaku, R B Olatunji, J A Balogun
{"title":"WHITE CEREBELLUM SIGN AS A DARK PROGNOSTIC INDICATOR OF CEREBRAL INJURY: A CASE REPORT.","authors":"O A Badejo, E C Nwafuluaku, R B Olatunji, J A Balogun","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The white cerebellum sign (WCS) is a classical but rare radiological finding usually associated with irreversible diffuse hypoxic-ischemic cerebral injury. Very few cases exist in the literature globally, especially from the West African region, as a potential hallmark of poor prognostic outcome. We describe the white cerebellum sign in a Nigerian pediatric patient, managed for severe head injury.</p><p><strong>Case presentation: </strong>A fourteen-year old boy presented to our emergency department with loss of consciousness following a pedestrian road traffic accident. Physical examination revealed a critically ill boy with fever, hypotension, tachycardia, gasping respiration, GCS 3, bilateral dilated unreactive pupils, absent corneal, gag and oculocephalic reflexes. He was thus diagnosed of severe traumatic brain injury and brainstem dysfunction. He had endotracheal intubation, ventilatory and inotropic support. Cranial computerized tomography scan of the patient showed radiological features in keeping with the WCS. His clinical status remained poor until he suffered a cardiac arrest about twelve hours after admission.</p><p><strong>Conclusion: </strong>WCS has been reported in relation to child abuse, anoxic-ischemic brain injury, inflammatory and metabolic brain disorders and trauma. It is a classical radiological description of diffuse cerebral edema alongside relatively normal cerebellar hemispheres and brainstem. Management of this pathology is symptomatic, and aims to ameliorate the associated raised intracranial pressure, control seizures and prevent cerebral infarction. The index patient, who presented 24 hours after severe head injury with associated early post-traumatic seizures, respiratory failure and brainstem dysfunction, had an unfavourable outcome consistent with previous reports of WCS. We have reported the rare but classical white cerebellum sign. It remains a grave prognosticator of cerebral injury and should be sought for in the neuroimaging of patients with acute brain insults.</p>","PeriodicalId":72221,"journal":{"name":"Annals of Ibadan postgraduate medicine","volume":"22 1","pages":"108-111"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11205724/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Ibadan postgraduate medicine","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: The white cerebellum sign (WCS) is a classical but rare radiological finding usually associated with irreversible diffuse hypoxic-ischemic cerebral injury. Very few cases exist in the literature globally, especially from the West African region, as a potential hallmark of poor prognostic outcome. We describe the white cerebellum sign in a Nigerian pediatric patient, managed for severe head injury.
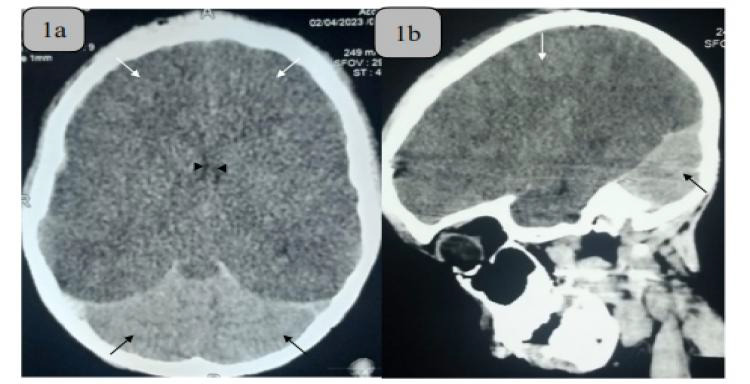
Case presentation: A fourteen-year old boy presented to our emergency department with loss of consciousness following a pedestrian road traffic accident. Physical examination revealed a critically ill boy with fever, hypotension, tachycardia, gasping respiration, GCS 3, bilateral dilated unreactive pupils, absent corneal, gag and oculocephalic reflexes. He was thus diagnosed of severe traumatic brain injury and brainstem dysfunction. He had endotracheal intubation, ventilatory and inotropic support. Cranial computerized tomography scan of the patient showed radiological features in keeping with the WCS. His clinical status remained poor until he suffered a cardiac arrest about twelve hours after admission.
Conclusion: WCS has been reported in relation to child abuse, anoxic-ischemic brain injury, inflammatory and metabolic brain disorders and trauma. It is a classical radiological description of diffuse cerebral edema alongside relatively normal cerebellar hemispheres and brainstem. Management of this pathology is symptomatic, and aims to ameliorate the associated raised intracranial pressure, control seizures and prevent cerebral infarction. The index patient, who presented 24 hours after severe head injury with associated early post-traumatic seizures, respiratory failure and brainstem dysfunction, had an unfavourable outcome consistent with previous reports of WCS. We have reported the rare but classical white cerebellum sign. It remains a grave prognosticator of cerebral injury and should be sought for in the neuroimaging of patients with acute brain insults.

 分享
分享



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
