{"title":"Risk factors at admission of in-hospital dysglycemia, mortality, and readmissions in patients with type 2 diabetes and pneumonia","authors":"Mikkel Thor Olsen , Carina Kirstine Klarskov , Katrine Bagge Hansen , Ulrik Pedersen-Bjergaard , Peter Lommer Kristensen","doi":"10.1016/j.jdiacomp.2024.108803","DOIUrl":null,"url":null,"abstract":"<div><h3>Aims</h3><p>In-hospital dysglycemia is associated with adverse outcomes. Identifying patients at risk of in-hospital dysglycemia early on admission may improve patient outcomes.</p></div><div><h3>Methods</h3><p>We analysed 117 inpatients admitted with pneumonia and type 2 diabetes monitored by continuous glucose monitoring. We assessed potential risk factors for in-hospital dysglycemia and adverse clinical outcomes.</p></div><div><h3>Results</h3><p>Time in range (3.9–10.0 mmol/l) decreased by 2.9 %-points [95 % CI 0.7–5.0] per 5 mmol/mol [2.6 %] increase in admission haemoglobin A1c, 16.2 %-points if admission diabetes therapy included insulin therapy [95 % CI 2.9–29.5], and 2.4 %-points [95 % CI 0.3–4.6] per increase in the Charlson Comorbidity Index (CCI) (integer, as a measure of severity and amount of comorbidities). Thirty-day readmission rate increased with an IRR of 1.24 [95 % CI 1.06–1.45] per increase in CCI. In-hospital mortality risk increased with an OR of 1.41 [95 % CI 1.07–1.87] per increase in Early Warning Score (EWS) (integer, as a measure of acute illness) at admission.</p></div><div><h3>Conclusions</h3><p>Dysglycemia among hospitalised patients with pneumonia and type 2 diabetes was associated with high haemoglobin A1c, insulin treatment before admission, and the amount and severity of comorbidities (i.e., CCI). Thirty-day readmission rate increased with high CCI. The risk of in-hospital mortality increased with the degree of acute illness (i.e., high EWS) at admission. Clinical outcomes were independent of chronic glycemic status, i.e. HbA1c, and in-hospital glycemic status.</p></div>","PeriodicalId":15659,"journal":{"name":"Journal of diabetes and its complications","volume":"38 8","pages":"Article 108803"},"PeriodicalIF":2.9000,"publicationDate":"2024-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S1056872724001296/pdfft?md5=117485bdd8f076b81ddb3b0a452d3c5e&pid=1-s2.0-S1056872724001296-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of diabetes and its complications","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1056872724001296","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Aims
In-hospital dysglycemia is associated with adverse outcomes. Identifying patients at risk of in-hospital dysglycemia early on admission may improve patient outcomes.
Methods
We analysed 117 inpatients admitted with pneumonia and type 2 diabetes monitored by continuous glucose monitoring. We assessed potential risk factors for in-hospital dysglycemia and adverse clinical outcomes.
Results
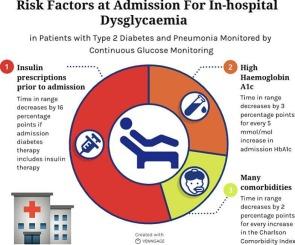
Time in range (3.9–10.0 mmol/l) decreased by 2.9 %-points [95 % CI 0.7–5.0] per 5 mmol/mol [2.6 %] increase in admission haemoglobin A1c, 16.2 %-points if admission diabetes therapy included insulin therapy [95 % CI 2.9–29.5], and 2.4 %-points [95 % CI 0.3–4.6] per increase in the Charlson Comorbidity Index (CCI) (integer, as a measure of severity and amount of comorbidities). Thirty-day readmission rate increased with an IRR of 1.24 [95 % CI 1.06–1.45] per increase in CCI. In-hospital mortality risk increased with an OR of 1.41 [95 % CI 1.07–1.87] per increase in Early Warning Score (EWS) (integer, as a measure of acute illness) at admission.
Conclusions
Dysglycemia among hospitalised patients with pneumonia and type 2 diabetes was associated with high haemoglobin A1c, insulin treatment before admission, and the amount and severity of comorbidities (i.e., CCI). Thirty-day readmission rate increased with high CCI. The risk of in-hospital mortality increased with the degree of acute illness (i.e., high EWS) at admission. Clinical outcomes were independent of chronic glycemic status, i.e. HbA1c, and in-hospital glycemic status.
期刊介绍:
Journal of Diabetes and Its Complications (JDC) is a journal for health care practitioners and researchers, that publishes original research about the pathogenesis, diagnosis and management of diabetes mellitus and its complications. JDC also publishes articles on physiological and molecular aspects of glucose homeostasis.
The primary purpose of JDC is to act as a source of information usable by diabetes practitioners and researchers to increase their knowledge about mechanisms of diabetes and complications development, and promote better management of people with diabetes who are at risk for those complications.
Manuscripts submitted to JDC can report any aspect of basic, translational or clinical research as well as epidemiology. Topics can range broadly from early prediabetes to late-stage complicated diabetes. Topics relevant to basic/translational reports include pancreatic islet dysfunction and insulin resistance, altered adipose tissue function in diabetes, altered neuronal control of glucose homeostasis and mechanisms of drug action. Topics relevant to diabetic complications include diabetic retinopathy, neuropathy and nephropathy; peripheral vascular disease and coronary heart disease; gastrointestinal disorders, renal failure and impotence; and hypertension and hyperlipidemia.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
