Zelin Ma, Yang Zhang, Han Han, Shengping Wang, Yuan Li, Haiquan Chen
{"title":"Segmentectomy versus lobectomy for ground-glass opacity dominant cT1N0 invasive lung adenocarcinoma.","authors":"Zelin Ma, Yang Zhang, Han Han, Shengping Wang, Yuan Li, Haiquan Chen","doi":"10.21037/tlcr-24-191","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Japan Clinical Oncology Group (JCOG) 1211 suggested that segmentectomy should be considered as standard treatment for clinical T1N0 (cT1N0) ground glass opacity (GGO). However, over half of patients in JCOG1211 had pre-/minimal invasive adenocarcinoma. This study aims to retrospectively investigate the long-term survival of GGO featured cT1N0 invasive lung adenocarcinoma undergoing segmentectomy or lobectomy.</p><p><strong>Methods: </strong>This study screened patients with primary cT1N0 lung adenocarcinoma who received segmentectomy or lobectomy from 2010-2020. Prior computed tomography (CT) scans before surgery of all patients were reviewed and the inclusion was confirmed according to tumor diameter and consolidation tumor ratio (CTR). GGO nodules between 2-3 cm with CTR ≤0.5 or ≤2 cm with CTR between 0.25-0.5 were finally included. Patients with pathologically diagnosed pre-/minimally invasive lung adenocarcinoma were excluded. Long-term survivals between segmentectomy group and lobectomy group were compared after propensity score matching (PSM). Recurrence and postoperative complication events were also analyzed.</p><p><strong>Results: </strong>In total, 617 patients were enrolled, 159 received segmentectomy and 458 received lobectomy. Clinicopathological characteristics were well distributed between two groups. With a median follow-up time of 61.1 months (IQR: 42.3-71.7 months), after PSM, the 5-year overall survival rate was 98.8% (97.9-99.6%) for lobectomy and 99.3% (98.2-99.8%) for segmentectomy (P=0.42), the 5-year relapse-free survival rate was 95.3% (92.2-97.6%) for lobectomy and 95.2% for segmentectomy (92.3-98.7%) (P=0.81). The proportion of recurrence was 4.1% for lobectomy and 4.4% for segmentectomy (P=0.89). The proportion of grade 2 and above early postoperative complications was 9.6% for lobectomy and 8.8% for segmentectomy (P=0.86).</p><p><strong>Conclusions: </strong>For cT1N0 GGO featured invasive lung adenocarcinoma (2 cm < tumor diameter ≤3 cm, CTR ≤0.5 or tumor diameter ≤2 cm, 0.25< CTR ≤0.5), postoperative outcomes between segmentectomy group and lobectomy group were comparable. Concerning minimally invasive surgical strategy, segmentectomy should be confirmed as the standard surgical approach.</p>","PeriodicalId":23271,"journal":{"name":"Translational lung cancer research","volume":"13 6","pages":"1201-1209"},"PeriodicalIF":3.5000,"publicationDate":"2024-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11225055/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Translational lung cancer research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/tlcr-24-191","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Japan Clinical Oncology Group (JCOG) 1211 suggested that segmentectomy should be considered as standard treatment for clinical T1N0 (cT1N0) ground glass opacity (GGO). However, over half of patients in JCOG1211 had pre-/minimal invasive adenocarcinoma. This study aims to retrospectively investigate the long-term survival of GGO featured cT1N0 invasive lung adenocarcinoma undergoing segmentectomy or lobectomy.
Methods: This study screened patients with primary cT1N0 lung adenocarcinoma who received segmentectomy or lobectomy from 2010-2020. Prior computed tomography (CT) scans before surgery of all patients were reviewed and the inclusion was confirmed according to tumor diameter and consolidation tumor ratio (CTR). GGO nodules between 2-3 cm with CTR ≤0.5 or ≤2 cm with CTR between 0.25-0.5 were finally included. Patients with pathologically diagnosed pre-/minimally invasive lung adenocarcinoma were excluded. Long-term survivals between segmentectomy group and lobectomy group were compared after propensity score matching (PSM). Recurrence and postoperative complication events were also analyzed.
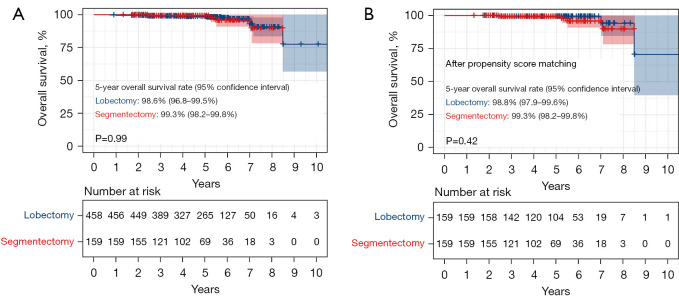
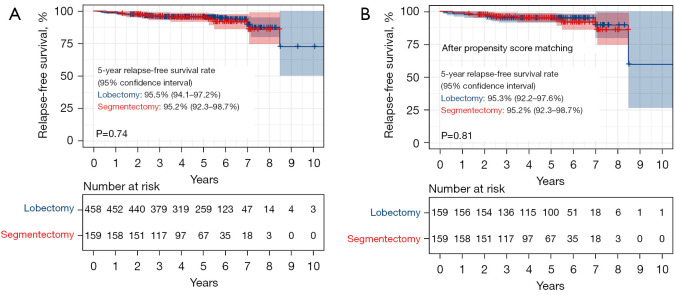
Results: In total, 617 patients were enrolled, 159 received segmentectomy and 458 received lobectomy. Clinicopathological characteristics were well distributed between two groups. With a median follow-up time of 61.1 months (IQR: 42.3-71.7 months), after PSM, the 5-year overall survival rate was 98.8% (97.9-99.6%) for lobectomy and 99.3% (98.2-99.8%) for segmentectomy (P=0.42), the 5-year relapse-free survival rate was 95.3% (92.2-97.6%) for lobectomy and 95.2% for segmentectomy (92.3-98.7%) (P=0.81). The proportion of recurrence was 4.1% for lobectomy and 4.4% for segmentectomy (P=0.89). The proportion of grade 2 and above early postoperative complications was 9.6% for lobectomy and 8.8% for segmentectomy (P=0.86).
Conclusions: For cT1N0 GGO featured invasive lung adenocarcinoma (2 cm < tumor diameter ≤3 cm, CTR ≤0.5 or tumor diameter ≤2 cm, 0.25< CTR ≤0.5), postoperative outcomes between segmentectomy group and lobectomy group were comparable. Concerning minimally invasive surgical strategy, segmentectomy should be confirmed as the standard surgical approach.
期刊介绍:
Translational Lung Cancer Research(TLCR, Transl Lung Cancer Res, Print ISSN 2218-6751; Online ISSN 2226-4477) is an international, peer-reviewed, open-access journal, which was founded in March 2012. TLCR is indexed by PubMed/PubMed Central and the Chemical Abstracts Service (CAS) Databases. It is published quarterly the first year, and published bimonthly since February 2013. It provides practical up-to-date information on prevention, early detection, diagnosis, and treatment of lung cancer. Specific areas of its interest include, but not limited to, multimodality therapy, markers, imaging, tumor biology, pathology, chemoprevention, and technical advances related to lung cancer.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
