An international multicentre study of SwiTching from Intravenous to subcutaneous inflixiMab and vEdolizumab in inflammatory bowel diseases: The TIME study
Ferdinando D'Amico, Luca Massimino, Giulia Palmieri, Arianna Dal Buono, Roberto Gabbiadini, Benedicte Caron, Paula Moreira, Isabel Silva, Maia Bosca-Watts, Tommaso Innocenti, Gabriele Dragoni, Cristina Bezzio, Alessandra Zilli, Federica Furfaro, Simone Saibeni, María Chaparro, María José García, George Michalopoulos, Nikos Viazis, Gerassimos J. Mantzaris, Pierre Ellul, Javier P. Gisbert, Fernando Magro, Laurent Peyrin-Biroulet, Alessandro Armuzzi, Federica Ungaro, Silvio Danese, Gionata Fiorino, Mariangela Allocca
{"title":"An international multicentre study of SwiTching from Intravenous to subcutaneous inflixiMab and vEdolizumab in inflammatory bowel diseases: The TIME study","authors":"Ferdinando D'Amico, Luca Massimino, Giulia Palmieri, Arianna Dal Buono, Roberto Gabbiadini, Benedicte Caron, Paula Moreira, Isabel Silva, Maia Bosca-Watts, Tommaso Innocenti, Gabriele Dragoni, Cristina Bezzio, Alessandra Zilli, Federica Furfaro, Simone Saibeni, María Chaparro, María José García, George Michalopoulos, Nikos Viazis, Gerassimos J. Mantzaris, Pierre Ellul, Javier P. Gisbert, Fernando Magro, Laurent Peyrin-Biroulet, Alessandro Armuzzi, Federica Ungaro, Silvio Danese, Gionata Fiorino, Mariangela Allocca","doi":"10.1111/eci.14283","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background and Aims</h3>\n \n <p>Subcutaneous (SC) formulations of infliximab (IFX) and vedolizumab (VDZ) are approved for the treatment of inflammatory bowel diseases (IBDs). Our aim was to evaluate the effectiveness of switching from intravenous (IV) to SC formulations of IFX and VDZ in IBDs.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This multicentre, retrospective study collected data of adult patients with Crohn's disease (CD) or ulcerative colitis (UC) switched to SC IFX or VDZ. The primary endpoint was clinical remission at 12 months stratified based on timing of switch. A composite endpoint consisting of therapy discontinuation, reverse-switch, need for steroids, and drug optimization was evaluated. A multivariate analysis investigated the association between patients' characteristics and outcomes.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Two hundred and thirty-one patients (59% UC, 53% male, mean age 44 ± 15 years, 68% IFX) from 13 centres were included. The switch occurred at Week 6 in a third of cases (36%). Median time to switch was 13 months. Most patients switched to SC IFX and VDZ were in clinical remission at 3 (87% and 77%), 6 (86% and 83%) and 12 (63% and 60%) months. In the multivariate analysis, there was no difference in clinical remission rate at 12 months; however, patients switched at Week 6 had a higher rate of experiencing any therapeutic changes at 3 (false discovery rate (FDR) = .002), 6 (FDR <1 × 10<sup>−10</sup>) or 12 months (FDR = .08). Clinical disease activity at baseline (only in UC) (FDR = .07) and previous exposure to biologics (FDR = .001) were risk factors for composite endpoint at 6 and 12 months.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>SC IFX and VDZ are effective in daily clinical practice in IBD patients. Switching patients in remission reduces the risk of negative outcomes.</p>\n </section>\n </div>","PeriodicalId":12013,"journal":{"name":"European Journal of Clinical Investigation","volume":"54 11","pages":""},"PeriodicalIF":3.6000,"publicationDate":"2024-07-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/eci.14283","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Clinical Investigation","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/eci.14283","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background and Aims
Subcutaneous (SC) formulations of infliximab (IFX) and vedolizumab (VDZ) are approved for the treatment of inflammatory bowel diseases (IBDs). Our aim was to evaluate the effectiveness of switching from intravenous (IV) to SC formulations of IFX and VDZ in IBDs.
Methods
This multicentre, retrospective study collected data of adult patients with Crohn's disease (CD) or ulcerative colitis (UC) switched to SC IFX or VDZ. The primary endpoint was clinical remission at 12 months stratified based on timing of switch. A composite endpoint consisting of therapy discontinuation, reverse-switch, need for steroids, and drug optimization was evaluated. A multivariate analysis investigated the association between patients' characteristics and outcomes.
Results
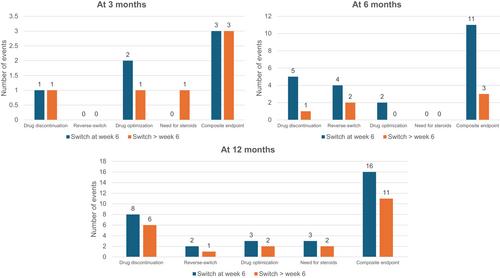
Two hundred and thirty-one patients (59% UC, 53% male, mean age 44 ± 15 years, 68% IFX) from 13 centres were included. The switch occurred at Week 6 in a third of cases (36%). Median time to switch was 13 months. Most patients switched to SC IFX and VDZ were in clinical remission at 3 (87% and 77%), 6 (86% and 83%) and 12 (63% and 60%) months. In the multivariate analysis, there was no difference in clinical remission rate at 12 months; however, patients switched at Week 6 had a higher rate of experiencing any therapeutic changes at 3 (false discovery rate (FDR) = .002), 6 (FDR <1 × 10−10) or 12 months (FDR = .08). Clinical disease activity at baseline (only in UC) (FDR = .07) and previous exposure to biologics (FDR = .001) were risk factors for composite endpoint at 6 and 12 months.
Conclusion
SC IFX and VDZ are effective in daily clinical practice in IBD patients. Switching patients in remission reduces the risk of negative outcomes.
期刊介绍:
EJCI considers any original contribution from the most sophisticated basic molecular sciences to applied clinical and translational research and evidence-based medicine across a broad range of subspecialties. The EJCI publishes reports of high-quality research that pertain to the genetic, molecular, cellular, or physiological basis of human biology and disease, as well as research that addresses prevalence, diagnosis, course, treatment, and prevention of disease. We are primarily interested in studies directly pertinent to humans, but submission of robust in vitro and animal work is also encouraged. Interdisciplinary work and research using innovative methods and combinations of laboratory, clinical, and epidemiological methodologies and techniques is of great interest to the journal. Several categories of manuscripts (for detailed description see below) are considered: editorials, original articles (also including randomized clinical trials, systematic reviews and meta-analyses), reviews (narrative reviews), opinion articles (including debates, perspectives and commentaries); and letters to the Editor.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
