Henrik Frisk, Oscar Persson, Michael Fagerlund, Margret Jensdottir, Victor Gabriel El-Hajj, Gustav Burström, Annika Sunesson, Annika Kits, Tomas Majing, Erik Edström, Magnus Kaijser, Adrian Elmi-Terander
{"title":"Intraoperative MRI without an intraoperative MRI suite: a workflow for glial tumor surgery.","authors":"Henrik Frisk, Oscar Persson, Michael Fagerlund, Margret Jensdottir, Victor Gabriel El-Hajj, Gustav Burström, Annika Sunesson, Annika Kits, Tomas Majing, Erik Edström, Magnus Kaijser, Adrian Elmi-Terander","doi":"10.1007/s00701-024-06165-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Intraoperative MRI (iMRI) has emerged as a useful tool in glioma surgery to safely improve the extent of resection. However, iMRI requires a dedicated operating room (OR) with an integrated MRI scanner solely for this purpose. Due to physical or economical restraints, this may not be feasible in all centers. The aim of this study was to investigate the feasibility of using a non-dedicated MRI scanner at the radiology department for iMRI and to describe the workflow with special focus on time expenditure and surgical implications.</p><p><strong>Methods: </strong>In total, 24 patients undergoing glioma surgery were included. When the resection was deemed completed, the wound was temporarily closed, and the patient, under general anesthesia, was transferred to the radiology department for iMRI, which was performed using a dedicated protocol on 1.5 or 3 T scanners. After performing iMRI the patient was returned to the OR for additional tumor resection or final wound closure. All procedural times, timestamps, and adverse events were recorded.</p><p><strong>Result: </strong>The median time from the decision to initiate iMRI until reopening of the wound after scanning was 68 (52-104) minutes. Residual tumors were found on iMRI in 13 patients (54%). There were no adverse events during the surgeries, transfers, transportations, or iMRI-examinations. There were no wound-related complications or infections in the postoperative period or at follow-up. There were no readmissions within 30 or 90 days due to any complication.</p><p><strong>Conclusion: </strong>Performing intraoperative MRI using an MRI located outside the OR department was feasible and safe with no adverse events. It did not require more time than previously reported data for dedicated iMRI scanners. This could be a viable alternative in centers without access to a dedicated iMRI suite.</p>","PeriodicalId":7370,"journal":{"name":"Acta Neurochirurgica","volume":"166 1","pages":"292"},"PeriodicalIF":1.9000,"publicationDate":"2024-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11236858/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta Neurochirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00701-024-06165-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Intraoperative MRI (iMRI) has emerged as a useful tool in glioma surgery to safely improve the extent of resection. However, iMRI requires a dedicated operating room (OR) with an integrated MRI scanner solely for this purpose. Due to physical or economical restraints, this may not be feasible in all centers. The aim of this study was to investigate the feasibility of using a non-dedicated MRI scanner at the radiology department for iMRI and to describe the workflow with special focus on time expenditure and surgical implications.
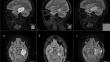
Methods: In total, 24 patients undergoing glioma surgery were included. When the resection was deemed completed, the wound was temporarily closed, and the patient, under general anesthesia, was transferred to the radiology department for iMRI, which was performed using a dedicated protocol on 1.5 or 3 T scanners. After performing iMRI the patient was returned to the OR for additional tumor resection or final wound closure. All procedural times, timestamps, and adverse events were recorded.
Result: The median time from the decision to initiate iMRI until reopening of the wound after scanning was 68 (52-104) minutes. Residual tumors were found on iMRI in 13 patients (54%). There were no adverse events during the surgeries, transfers, transportations, or iMRI-examinations. There were no wound-related complications or infections in the postoperative period or at follow-up. There were no readmissions within 30 or 90 days due to any complication.
Conclusion: Performing intraoperative MRI using an MRI located outside the OR department was feasible and safe with no adverse events. It did not require more time than previously reported data for dedicated iMRI scanners. This could be a viable alternative in centers without access to a dedicated iMRI suite.
期刊介绍:
The journal "Acta Neurochirurgica" publishes only original papers useful both to research and clinical work. Papers should deal with clinical neurosurgery - diagnosis and diagnostic techniques, operative surgery and results, postoperative treatment - or with research work in neuroscience if the underlying questions or the results are of neurosurgical interest. Reports on congresses are given in brief accounts. As official organ of the European Association of Neurosurgical Societies the journal publishes all announcements of the E.A.N.S. and reports on the activities of its member societies. Only contributions written in English will be accepted.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
