Prognostic Strength of CA 19-9, Demographic Parameters, and Maximum Standardized Uptake Value of Baseline 18F-FDG PET/CT in Treatment-naïve Patients with Pancreatic Carcinoma.
Nosheen Fatima, Unaiza Zaman, Areeba Zaman, Sidra Zaman, Rabia Tahseen, Maseeh Uz Zaman
{"title":"Prognostic Strength of CA 19-9, Demographic Parameters, and Maximum Standardized Uptake Value of Baseline 18F-FDG PET/CT in Treatment-naïve Patients with Pancreatic Carcinoma.","authors":"Nosheen Fatima, Unaiza Zaman, Areeba Zaman, Sidra Zaman, Rabia Tahseen, Maseeh Uz Zaman","doi":"10.4103/ijnm.ijnm_6_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim and background: </strong>The aim of this study was to evaluate the prognostic value of imaging-based variables and tumor marker in predicting the progression-free survival (PFS) in treatment-naïve pancreatic cancer (PC) using baseline 18-fluorodeoxyglucose (<sup>18</sup>FDG) positron emission tomography/computed tomography (PET/CT).</p><p><strong>Materials and methods: </strong>This retro-prospective study was conducted at PET/CT imaging facility of JCIA health-care facility of Pakistan. Total 68 patients with PCs were retrospectively included who had <sup>18</sup>FDG PET/CT for staging from March 2017 to December 2020. Thirty-two patients had unresectable Stage IV disease on baseline imaging while the remaining 36 underwent Whipple's procedure and both categories were followed by chemotherapy with/without immunotherapy. These patients were followed for a median period of 18 months (1-62 months) for PFS. Logistic regression analysis and receiver operating characteristic (ROC) analysis were used for independent predictors of patients' demographics, tumor characteristics, CA 19-9, and maximum standardized uptake value (SUVmax) in PFS. Kaplan-Meier's survival curves were analyzed to measure PFS using ROC-derived significant cutoff values of CA 19-9 and SUVmax.</p><p><strong>Results: </strong>Median PFS was 18 months (11-45) with 60% (41/68) patients were either died or labelled having metabolic progressive disease (MPD. Using logistic regression analysis, significant correlations were found for Stage IV disease and pancreatic body/tail tumor with disease progression (odd ratio: 7.535 and 4.803, respectively; <i>P</i> < 0.05). Gender, obesity, histological tumor type, and <sup>18</sup>FDG-avid regional nodes did not show a significant impact on PFS. On ROC analysis, SUVmax >5.3 of primary tumor and baseline CA 19-9 >197 U/ml were found to have a significant negative correlation with PFS (area under the curve: 0.827 and 0.911, respectively; <i>P</i> < 0.0001) and no association of age and primary tumor size in PFS. Significantly, shorter PFS was found using ROC-derived cutoff values of SUVmax >5.3 versus ≤5.3 of primary tumor (mean and 95% confidence interval [CI]: 16.7 vs. 48.5 and 10-23 vs. 41-56; log-rank = 25.014; <i>P</i> < 0.0001) and baseline CA 19-9 >197 versus ≤197 U/ml (mean and 95% CI: 11.8 vs. 46.9 and 7-16 vs. 39-55; log-rank = 38.217; <i>P</i> < 0.0001).</p><p><strong>Conclusion: </strong>SUVmax >5.3 of primary tumor and baseline CA 19-9 >197 U/ml were found to have a significant negative correlation with PFS in treatment-naïve PC patients. Among demographics, only Stage IV disease and pancreatic tail and body tumors were found to have a negative association with disease progression.</p>","PeriodicalId":45830,"journal":{"name":"Indian Journal of Nuclear Medicine","volume":"39 2","pages":"77-82"},"PeriodicalIF":0.5000,"publicationDate":"2024-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11232728/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Indian Journal of Nuclear Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/ijnm.ijnm_6_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/5/29 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Aim and background: The aim of this study was to evaluate the prognostic value of imaging-based variables and tumor marker in predicting the progression-free survival (PFS) in treatment-naïve pancreatic cancer (PC) using baseline 18-fluorodeoxyglucose (18FDG) positron emission tomography/computed tomography (PET/CT).
Materials and methods: This retro-prospective study was conducted at PET/CT imaging facility of JCIA health-care facility of Pakistan. Total 68 patients with PCs were retrospectively included who had 18FDG PET/CT for staging from March 2017 to December 2020. Thirty-two patients had unresectable Stage IV disease on baseline imaging while the remaining 36 underwent Whipple's procedure and both categories were followed by chemotherapy with/without immunotherapy. These patients were followed for a median period of 18 months (1-62 months) for PFS. Logistic regression analysis and receiver operating characteristic (ROC) analysis were used for independent predictors of patients' demographics, tumor characteristics, CA 19-9, and maximum standardized uptake value (SUVmax) in PFS. Kaplan-Meier's survival curves were analyzed to measure PFS using ROC-derived significant cutoff values of CA 19-9 and SUVmax.
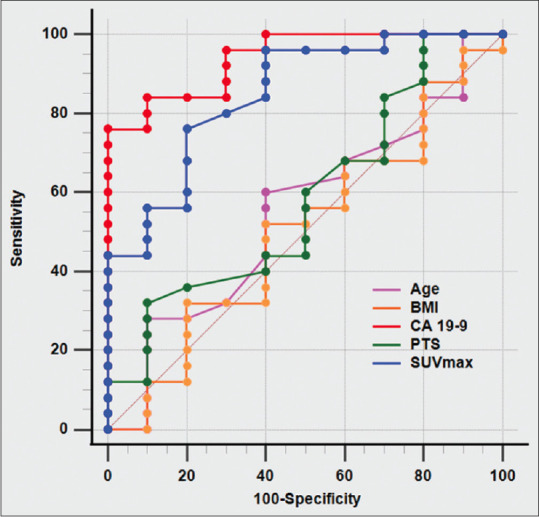
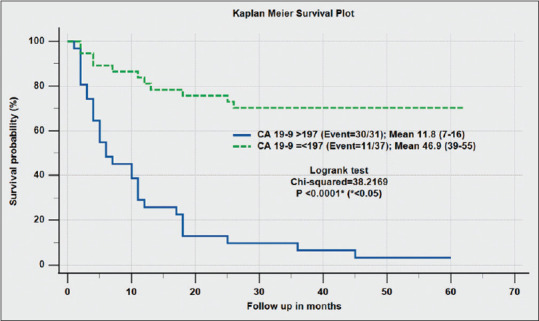
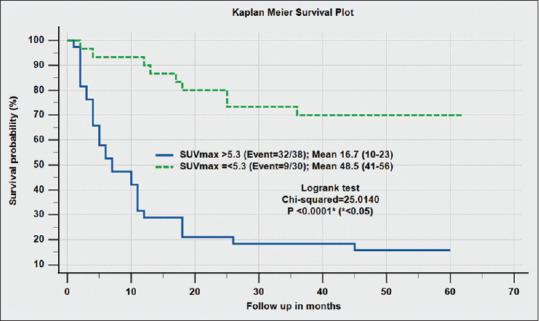
Results: Median PFS was 18 months (11-45) with 60% (41/68) patients were either died or labelled having metabolic progressive disease (MPD. Using logistic regression analysis, significant correlations were found for Stage IV disease and pancreatic body/tail tumor with disease progression (odd ratio: 7.535 and 4.803, respectively; P < 0.05). Gender, obesity, histological tumor type, and 18FDG-avid regional nodes did not show a significant impact on PFS. On ROC analysis, SUVmax >5.3 of primary tumor and baseline CA 19-9 >197 U/ml were found to have a significant negative correlation with PFS (area under the curve: 0.827 and 0.911, respectively; P < 0.0001) and no association of age and primary tumor size in PFS. Significantly, shorter PFS was found using ROC-derived cutoff values of SUVmax >5.3 versus ≤5.3 of primary tumor (mean and 95% confidence interval [CI]: 16.7 vs. 48.5 and 10-23 vs. 41-56; log-rank = 25.014; P < 0.0001) and baseline CA 19-9 >197 versus ≤197 U/ml (mean and 95% CI: 11.8 vs. 46.9 and 7-16 vs. 39-55; log-rank = 38.217; P < 0.0001).
Conclusion: SUVmax >5.3 of primary tumor and baseline CA 19-9 >197 U/ml were found to have a significant negative correlation with PFS in treatment-naïve PC patients. Among demographics, only Stage IV disease and pancreatic tail and body tumors were found to have a negative association with disease progression.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
