Agathe M de Pins, Dorothy Adu-Amankwah, Kristin A Shadman, Skylar M Hess, Cordelia R Elaiho, Liam R Butler, Sheena C Ranade, Brijen J Shah, Robert Fields, Elaine P Lin
{"title":"A Quality Improvement Project to Improve After-visit Summary Patient Instructions in a Pediatric Multidisciplinary Neuromuscular Program.","authors":"Agathe M de Pins, Dorothy Adu-Amankwah, Kristin A Shadman, Skylar M Hess, Cordelia R Elaiho, Liam R Butler, Sheena C Ranade, Brijen J Shah, Robert Fields, Elaine P Lin","doi":"10.1097/pq9.0000000000000743","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Multidisciplinary clinics aim to coordinate care between multiple specialties for children with medical complexity yet may result in information overload for caregivers. The after-visit summary (AVS) patient instruction section offers a solution by summarizing visit details and recommendations. No known studies address patient instruction optimization and integration within a multidisciplinary clinic setting. This project aimed to improve the quality of patient instructions to support better postvisit communication between caregivers and providers in a multidisciplinary pediatric neuromuscular program.</p><p><strong>Methods: </strong>A multidisciplinary stakeholder team created a key driver diagram to improve postvisit communication between caregivers and providers in the clinic. The first specific aim was to achieve an 80% completion rate of AVS patient instructions within 6 months. To do so, a standardized electronic medical record \"text shortcut\" was created for consistent information in each patient's instructions. Feedback on AVS from caregivers was obtained using the Family Experiences with Coordination of Care survey and open-ended interviews. This feedback informed the next specific aim: to reduce medical jargon within patient instructions by 25% over 3 months. Completion rates and jargon use were reviewed using control charts.</p><p><strong>Results: </strong>AVS patient instruction completion rates increased from a mean of 39.4%-85.0%. Provider education reduced mean jargon usage in patient instructions, from 8.2 to 3.9 jargon terms.</p><p><strong>Conclusions: </strong>Provider education and caregiver feedback helped improve patient communication by enhancing AVS compliance and diminishing medical jargon. Interventions to improve AVS patient instructions may enhance patient communication strategies for complex medical visits.</p>","PeriodicalId":74412,"journal":{"name":"Pediatric quality & safety","volume":"9 4","pages":"e743"},"PeriodicalIF":1.1000,"publicationDate":"2024-07-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11236396/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric quality & safety","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/pq9.0000000000000743","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Multidisciplinary clinics aim to coordinate care between multiple specialties for children with medical complexity yet may result in information overload for caregivers. The after-visit summary (AVS) patient instruction section offers a solution by summarizing visit details and recommendations. No known studies address patient instruction optimization and integration within a multidisciplinary clinic setting. This project aimed to improve the quality of patient instructions to support better postvisit communication between caregivers and providers in a multidisciplinary pediatric neuromuscular program.
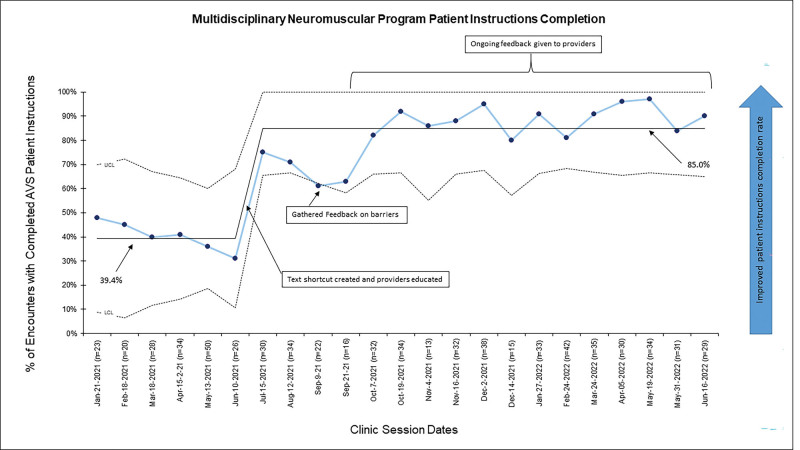
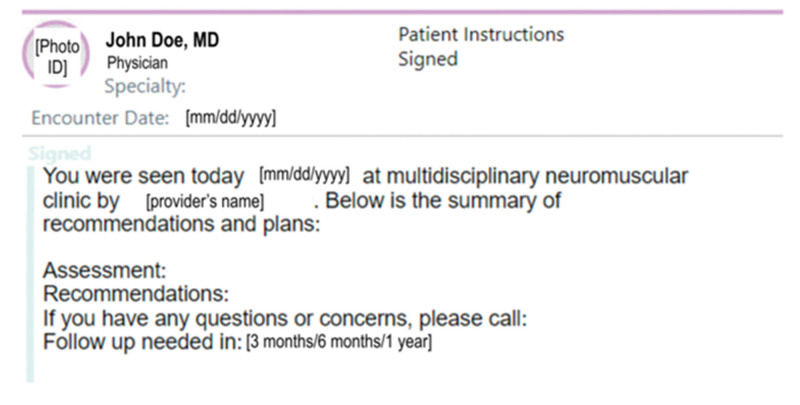
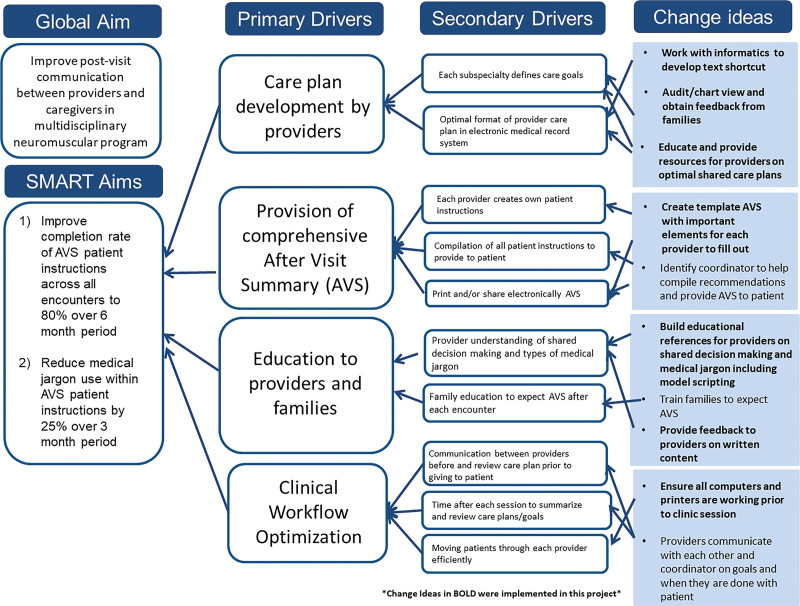
Methods: A multidisciplinary stakeholder team created a key driver diagram to improve postvisit communication between caregivers and providers in the clinic. The first specific aim was to achieve an 80% completion rate of AVS patient instructions within 6 months. To do so, a standardized electronic medical record "text shortcut" was created for consistent information in each patient's instructions. Feedback on AVS from caregivers was obtained using the Family Experiences with Coordination of Care survey and open-ended interviews. This feedback informed the next specific aim: to reduce medical jargon within patient instructions by 25% over 3 months. Completion rates and jargon use were reviewed using control charts.
Results: AVS patient instruction completion rates increased from a mean of 39.4%-85.0%. Provider education reduced mean jargon usage in patient instructions, from 8.2 to 3.9 jargon terms.
Conclusions: Provider education and caregiver feedback helped improve patient communication by enhancing AVS compliance and diminishing medical jargon. Interventions to improve AVS patient instructions may enhance patient communication strategies for complex medical visits.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
