Ibrahim Ben Razek MD, Maria Isabel Vargas MD, Daniel S. Schechter MD, Margitta Seeck MD
{"title":"Newly Developed Craving for Swiss Chocolate","authors":"Ibrahim Ben Razek MD, Maria Isabel Vargas MD, Daniel S. Schechter MD, Margitta Seeck MD","doi":"10.1002/ana.27023","DOIUrl":null,"url":null,"abstract":"<p>Craving, addiction, and compulsive eating leading to obesity are major public health problems incurring estimated direct and indirect costs of up to $600 billion.<span><sup>1</sup></span> The opioid crisis, declared as a public health emergency in 2017, showed that there is still insufficient understanding of craving, thereby hampering the ability to treat it effectively. Studies have strived to identify the neuronal correlates of addiction,<span><sup>2</sup></span> leading to the isolation of brain networks mainly based in the frontal lobe. Evidence from experimental animal and human studies have suggested a major role of the orbito-frontal cortex (OFC).<span><sup>2, 3</sup></span> However, to our knowledge, there are no reports of new-onset craving due to a circumscribed lesion that corroborate this notion. This report presents the first case of craving, targeting Swiss chocolate, due to minor postoperative fronto-orbital bleeding, dissipating over time as the lesion disappeared.</p><p>A patient aged in his 50s, right-handed, with an unremarkable medical and psychiatric history was admitted to the emergency department after a first generalized epileptic seizure. Brain magnetic resonance imaging showed a voluminous mass suggesting a frontobasal meningioma with surrounding edema (Fig 1A). He was prescribed levetiracetam 500 mg b.i.d. Four days later, he underwent neurosurgery with complete tumor resection, leaving a small compressive hematoma in the left OFC (Fig 1B–D). Histopathology confirmed a meningioma, World Health Organization grade I. He left hospital after 9 days with a normal physical examination. To determine if his antiseizure medication (levetiracetam) could be discontinued, he was referred to ambulatory epileptology.</p><p>There were no further seizures or suspicious events, awake or asleep. Levetiracetam was well tolerated.</p><p>Two weeks after surgery, the patient started to notice a strong craving for chocolate, particularly, Swiss dark chocolate with hazelnuts, and had to consume at least 200–300 g daily. He became irritable and nervous if his wife did not purchase this special type of chocolate, and would search for it throughout metropolitan Geneva, even after shops closed (eg, driving 30 min to the airport to buy this specific chocolate). He never lost control (eg, became physically violent) or suffered from significant withdrawal symptoms (eg, sweating) from his newly developed craving. However, he would rant and rail at his family if he did not get his chocolate.</p><p>Before neurosurgery, the patient's desire for chocolate was not particularly strong. He did not smoke, and only drank alcohol occasionally. He would ride his bike regularly, without changes in the frequency or intensity of his physical activity from the time before to the time after the operation. He impressed the neurology team with his slim, sporty figure without evidence of weight gain.</p><p>His chocolate craving decreased gradually 4 months postoperatively, and completely disappeared within a year. A control magnetic resonance imaging was carried out 6 months after the operation and showed significant regression of the hematoma (Fig 1E,F). Levetiracetam was discontinued, without seizure recurrence during 3 years follow-up or onset of any other neurological or psychiatric illness.</p><p>To our knowledge, this is the first clinical report of craving due to a lesion in the OFC, leading to psychophysiological withdrawal symptoms if his “fix” (here, chocolate) was low. Craving appeared as a consequence of the surgical intervention in the OFC, which led to a small hematoma in the left mesial fronto-basal cortex that spontaneously resolved within 6 months. Its disappearance coincided with the resolution of the craving symptoms.</p><p>It is well established that patients with frontotemporal dementia present personality changes, including impulsive and repetitive behavior.<span><sup>4</sup></span> However, addiction and compulsive behavior rely on a particular network of key structures, which involves mainly the frontal lobe; that is, the ventromedial and dorsolateral prefrontal cortex, anterior cingulate gyrus, and the OFC.<span><sup>2</sup></span> Synaptic potentiation of transmission from the OFC to the dorsal striatum represents a neural correlate that drives compulsive reinforcement, a defining symptom of craving and addiction.<span><sup>3</sup></span></p><p>In a study of healthy chocolate consumers, altered activity was found in the medial OFC,<span><sup>5</sup></span> concordant with the lesion site of the present patient. Hypoactivity in the OFC, as it is the case with acute lesions, appears to be the basis for repetitive compulsive behavior.<span><sup>2</sup></span> Imaging studies have revealed decreases in the orbitofrontal and anterior cingulate cortex during dependence, and reactivation during acute craving episodes.<span><sup>2</sup></span> Although chocolate (or food in general), alcohol, and heroin craving differ significantly in various neurobiological and societal aspects, the subserving anatomical network seems to be similar and implicates the OFC.</p><p>An alternative explanation of our patient's new chocolate addiction could be the tumor itself. Yet, as meningioma type I grow very slowly, chocolate craving should have been present before the operation. As aforementioned, the patient showed no particular interest in chocolate before his neurosurgery.</p><p>The transient lesion's origin was identified in the left-sided mesial OFC, despite the literature supporting no lateralized neural correlates of craving. Deep brain stimulation addiction studies, furthermore, target both hemispheres.<span><sup>6</sup></span> New onset obsessive-compulsive disorder followed by bleeding were described in the left frontal lobe,<span><sup>7</sup></span> whereas right anterior dominance was noted for the “Gourmand syndrome,” a newly developed strong interest for high-quality food after stroke or traumatic brain injury.<span><sup>8</sup></span> The present case involved bilateral lesions due to postoperative edema and a left-sided hematoma.</p><p>Food craving is probably the most frequent compulsive behavior worldwide, with significant morbidity associated. A recent review of 19 randomized control trials of noninvasive brain stimulation suggested that active stimulation of the dorsolateral prefrontal cortex resulted in lower body mass index and food craving.<span><sup>9</sup></span> For anatomical reasons, the mesial OFC is difficult to reach by noninvasive stimulation, but a recent study showed that these constraints might be overcome with appropriate anatomical targeting,<span><sup>10</sup></span> opening new therapeutic avenues for those unable to control their compulsions.</p><p>Careful clinical studies of patients with new distinct lesions in different parts of the OFC are necessary to learn more about neural correlates of compulsive behavior, craving, and addiction in humans. Such a knowledge may help to design more effective personalized treatment options to cope with the large number of people suffering from persistent compulsions and addictions with their ensuing costs to society, of which craving for food is worldwide the most prevailing.</p><p>All authors contributed to the conception and design of the manuscript. I.B.R. and M.S. were in charge of data acquisition and preparation of figures. All authors contributed to reviewing/editing and final approval of the manuscript.</p><p>Nothing to report.</p>","PeriodicalId":127,"journal":{"name":"Annals of Neurology","volume":"96 4","pages":"675-677"},"PeriodicalIF":7.7000,"publicationDate":"2024-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ana.27023","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Neurology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ana.27023","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Craving, addiction, and compulsive eating leading to obesity are major public health problems incurring estimated direct and indirect costs of up to $600 billion.1 The opioid crisis, declared as a public health emergency in 2017, showed that there is still insufficient understanding of craving, thereby hampering the ability to treat it effectively. Studies have strived to identify the neuronal correlates of addiction,2 leading to the isolation of brain networks mainly based in the frontal lobe. Evidence from experimental animal and human studies have suggested a major role of the orbito-frontal cortex (OFC).2, 3 However, to our knowledge, there are no reports of new-onset craving due to a circumscribed lesion that corroborate this notion. This report presents the first case of craving, targeting Swiss chocolate, due to minor postoperative fronto-orbital bleeding, dissipating over time as the lesion disappeared.
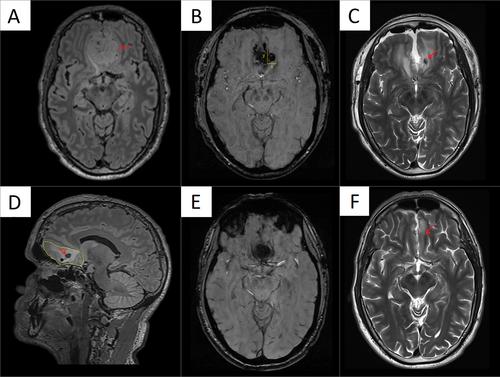
A patient aged in his 50s, right-handed, with an unremarkable medical and psychiatric history was admitted to the emergency department after a first generalized epileptic seizure. Brain magnetic resonance imaging showed a voluminous mass suggesting a frontobasal meningioma with surrounding edema (Fig 1A). He was prescribed levetiracetam 500 mg b.i.d. Four days later, he underwent neurosurgery with complete tumor resection, leaving a small compressive hematoma in the left OFC (Fig 1B–D). Histopathology confirmed a meningioma, World Health Organization grade I. He left hospital after 9 days with a normal physical examination. To determine if his antiseizure medication (levetiracetam) could be discontinued, he was referred to ambulatory epileptology.
There were no further seizures or suspicious events, awake or asleep. Levetiracetam was well tolerated.
Two weeks after surgery, the patient started to notice a strong craving for chocolate, particularly, Swiss dark chocolate with hazelnuts, and had to consume at least 200–300 g daily. He became irritable and nervous if his wife did not purchase this special type of chocolate, and would search for it throughout metropolitan Geneva, even after shops closed (eg, driving 30 min to the airport to buy this specific chocolate). He never lost control (eg, became physically violent) or suffered from significant withdrawal symptoms (eg, sweating) from his newly developed craving. However, he would rant and rail at his family if he did not get his chocolate.
Before neurosurgery, the patient's desire for chocolate was not particularly strong. He did not smoke, and only drank alcohol occasionally. He would ride his bike regularly, without changes in the frequency or intensity of his physical activity from the time before to the time after the operation. He impressed the neurology team with his slim, sporty figure without evidence of weight gain.
His chocolate craving decreased gradually 4 months postoperatively, and completely disappeared within a year. A control magnetic resonance imaging was carried out 6 months after the operation and showed significant regression of the hematoma (Fig 1E,F). Levetiracetam was discontinued, without seizure recurrence during 3 years follow-up or onset of any other neurological or psychiatric illness.
To our knowledge, this is the first clinical report of craving due to a lesion in the OFC, leading to psychophysiological withdrawal symptoms if his “fix” (here, chocolate) was low. Craving appeared as a consequence of the surgical intervention in the OFC, which led to a small hematoma in the left mesial fronto-basal cortex that spontaneously resolved within 6 months. Its disappearance coincided with the resolution of the craving symptoms.
It is well established that patients with frontotemporal dementia present personality changes, including impulsive and repetitive behavior.4 However, addiction and compulsive behavior rely on a particular network of key structures, which involves mainly the frontal lobe; that is, the ventromedial and dorsolateral prefrontal cortex, anterior cingulate gyrus, and the OFC.2 Synaptic potentiation of transmission from the OFC to the dorsal striatum represents a neural correlate that drives compulsive reinforcement, a defining symptom of craving and addiction.3
In a study of healthy chocolate consumers, altered activity was found in the medial OFC,5 concordant with the lesion site of the present patient. Hypoactivity in the OFC, as it is the case with acute lesions, appears to be the basis for repetitive compulsive behavior.2 Imaging studies have revealed decreases in the orbitofrontal and anterior cingulate cortex during dependence, and reactivation during acute craving episodes.2 Although chocolate (or food in general), alcohol, and heroin craving differ significantly in various neurobiological and societal aspects, the subserving anatomical network seems to be similar and implicates the OFC.
An alternative explanation of our patient's new chocolate addiction could be the tumor itself. Yet, as meningioma type I grow very slowly, chocolate craving should have been present before the operation. As aforementioned, the patient showed no particular interest in chocolate before his neurosurgery.
The transient lesion's origin was identified in the left-sided mesial OFC, despite the literature supporting no lateralized neural correlates of craving. Deep brain stimulation addiction studies, furthermore, target both hemispheres.6 New onset obsessive-compulsive disorder followed by bleeding were described in the left frontal lobe,7 whereas right anterior dominance was noted for the “Gourmand syndrome,” a newly developed strong interest for high-quality food after stroke or traumatic brain injury.8 The present case involved bilateral lesions due to postoperative edema and a left-sided hematoma.
Food craving is probably the most frequent compulsive behavior worldwide, with significant morbidity associated. A recent review of 19 randomized control trials of noninvasive brain stimulation suggested that active stimulation of the dorsolateral prefrontal cortex resulted in lower body mass index and food craving.9 For anatomical reasons, the mesial OFC is difficult to reach by noninvasive stimulation, but a recent study showed that these constraints might be overcome with appropriate anatomical targeting,10 opening new therapeutic avenues for those unable to control their compulsions.
Careful clinical studies of patients with new distinct lesions in different parts of the OFC are necessary to learn more about neural correlates of compulsive behavior, craving, and addiction in humans. Such a knowledge may help to design more effective personalized treatment options to cope with the large number of people suffering from persistent compulsions and addictions with their ensuing costs to society, of which craving for food is worldwide the most prevailing.
All authors contributed to the conception and design of the manuscript. I.B.R. and M.S. were in charge of data acquisition and preparation of figures. All authors contributed to reviewing/editing and final approval of the manuscript.
期刊介绍:
Annals of Neurology publishes original articles with potential for high impact in understanding the pathogenesis, clinical and laboratory features, diagnosis, treatment, outcomes and science underlying diseases of the human nervous system. Articles should ideally be of broad interest to the academic neurological community rather than solely to subspecialists in a particular field. Studies involving experimental model system, including those in cell and organ cultures and animals, of direct translational relevance to the understanding of neurological disease are also encouraged.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
