Ming Wai Yeung , M. Abdullah Said , Yordi J. van de Vegte , Niek Verweij , Robin P.F. Dullaart , Pim van der Harst
{"title":"Associations of very low Lipoprotein(a) levels with risks of new-onset diabetes and non-alcoholic liver disease","authors":"Ming Wai Yeung , M. Abdullah Said , Yordi J. van de Vegte , Niek Verweij , Robin P.F. Dullaart , Pim van der Harst","doi":"10.1016/j.athplu.2024.07.001","DOIUrl":null,"url":null,"abstract":"<div><h3>Background and aims</h3><p>We aimed to study the association of very low serum Lipoprotein(a) [Lp(a)] concentrations with new-onset type 2 diabetes (T2D) and non-alcoholic liver disease (NAFLD) in the context of statin usage in the UK Biobank, a large prospective population cohort.</p></div><div><h3>Methods</h3><p>Using an extended biomarker dataset, we identified 47,362 participants with very low Lp(a) concentrations (<3.8 nmol/L) from a total of 451,479 participants. With a median follow-up of 12.3 years, we assessed the risk of new-onset cardiometabolic diseases in participants stratified by statin usage with Cox proportional hazards models. We performed two-sample Mendelian randomization MR analyses to test causal relationship between genetically predicted Lp(a) and T2D and NAFLD.</p></div><div><h3>Results</h3><p>Taking the participants with Lp(a) within reportable range as the reference group, the hazard ratios (HR) for T2D were 1.07 (95 % confidence interval, CI 1.01–1.13) and for NAFLD 1.30 (95 % CI 1.20–1.41) respectively for participants with very low Lp(a) (<3.8 nmol/L). The risk for new-onset T2D was higher in participants using statins (adjusted HR 1.15; 95 % CI 1.05–1.27). The risk estimates for new-onset NAFLD were comparable in the analysis stratified by statin use. There was no evidence for causal links between genetically predicted Lp(a) and T2D nor NAFLD in two-sample MR analyses.</p></div><div><h3>Conclusions</h3><p>Very low Lp(a) was associated with higher risks of T2D and NAFLD in a prospective analysis of the UK Biobank. The association with T2D was influenced by lipid lowering medication usage. MR analyses did not support causality for these inverse associations.</p></div>","PeriodicalId":72324,"journal":{"name":"Atherosclerosis plus","volume":"57 ","pages":"Pages 19-25"},"PeriodicalIF":2.1000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2667089524000166/pdfft?md5=c3a6777b13986ebec4c5e9321f64810d&pid=1-s2.0-S2667089524000166-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Atherosclerosis plus","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2667089524000166","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Background and aims
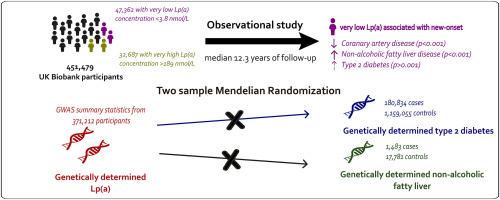
We aimed to study the association of very low serum Lipoprotein(a) [Lp(a)] concentrations with new-onset type 2 diabetes (T2D) and non-alcoholic liver disease (NAFLD) in the context of statin usage in the UK Biobank, a large prospective population cohort.
Methods
Using an extended biomarker dataset, we identified 47,362 participants with very low Lp(a) concentrations (<3.8 nmol/L) from a total of 451,479 participants. With a median follow-up of 12.3 years, we assessed the risk of new-onset cardiometabolic diseases in participants stratified by statin usage with Cox proportional hazards models. We performed two-sample Mendelian randomization MR analyses to test causal relationship between genetically predicted Lp(a) and T2D and NAFLD.
Results
Taking the participants with Lp(a) within reportable range as the reference group, the hazard ratios (HR) for T2D were 1.07 (95 % confidence interval, CI 1.01–1.13) and for NAFLD 1.30 (95 % CI 1.20–1.41) respectively for participants with very low Lp(a) (<3.8 nmol/L). The risk for new-onset T2D was higher in participants using statins (adjusted HR 1.15; 95 % CI 1.05–1.27). The risk estimates for new-onset NAFLD were comparable in the analysis stratified by statin use. There was no evidence for causal links between genetically predicted Lp(a) and T2D nor NAFLD in two-sample MR analyses.
Conclusions
Very low Lp(a) was associated with higher risks of T2D and NAFLD in a prospective analysis of the UK Biobank. The association with T2D was influenced by lipid lowering medication usage. MR analyses did not support causality for these inverse associations.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
