Shreesha Kumar Kodavoor, Ashalyne James Joseph, Shreyas Ramamurthy, Ramamurthy Dandapani
{"title":"Management of pterygium: our experience and a simplified treatment algorithm.","authors":"Shreesha Kumar Kodavoor, Ashalyne James Joseph, Shreyas Ramamurthy, Ramamurthy Dandapani","doi":"10.22336/rjo.2024.21","DOIUrl":null,"url":null,"abstract":"<p><p><b>Aim:</b> To explore various approaches in the management of pterygium and to propose a simplified treatment algorithm for its surgical management. <b>Methods:</b> A retrospective analysis of 9219 eyes was done. Group I included patients with primary single-head pterygium, most undergoing pterygium excision with conjunctival autograft (CAG). CTG-P (Conjunctival tissue graft from pterygium), AMG (Amniotic membrane graft), and inferior CAG were done in the remaining patients in this group in which conventional conjunctival autograft was a relative contraindication. Group II included patients with primary double-head pterygium who underwent vertical/horizontal split CAG, with/without limbal orientation, Inferior + Superior CAG, CTG-P, and CAG + CTG-P. Group III included patients with recurrent single-head pterygium who underwent ER (Extended resection) + LCAG (Limbal conjunctival autograft), LCAG + MMC (Mitomycin-C), CAG + MMC (Mitomycin-C) and CAG. Group IV included patients with recurrent double-head pterygium who underwent split LCAG and CAG + SLET. <b>Results:</b> All the four groups reported a low incidence of pterygium recurrence. Recurrence was observed at a rate of 0.47%, 3.63%, 2.86%, and 7.69% in Group I, Group II, Group III and Group IV respectively. <b>Discussion:</b> We mainly aimed to get minimal recurrence and good cosmetic outcomes. In double-head pterygium, we could achieve good and comparable outcomes with horizontal or vertical split CAG, with or without maintaining limbal orientation. Similarly, Inferior + Superior CAG, CTG-P, CAG+CTG-P, and AMG also showed low recurrence rates. In recurrent pterygium, ER + LCAG/CAG, with/without adjuncts like MMC showed low recurrence rates. Thus, all of these methods were found to be viable options. The main strength of our study, compared to previous studies on pterygium was its large sample size and long duration of follow-up. <b>Conclusion:</b> All the methods we studied had a low recurrence rate. We have formulated a treatment algorithm for pterygium management based on our outcomes. <b>Abbreviations:</b> CAG = Conjunctival autograft, CTG-P = Conjunctival tissue graft from pterygium, ER = Extended resection, MMC = Mitomycin-C.</p>","PeriodicalId":94355,"journal":{"name":"Romanian journal of ophthalmology","volume":"68 2","pages":"108-113"},"PeriodicalIF":0.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11238865/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Romanian journal of ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22336/rjo.2024.21","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
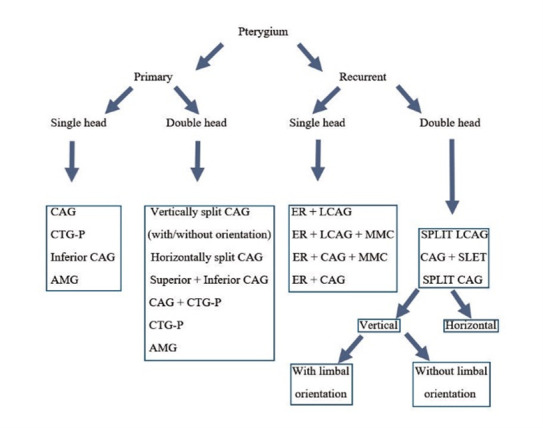
Aim: To explore various approaches in the management of pterygium and to propose a simplified treatment algorithm for its surgical management. Methods: A retrospective analysis of 9219 eyes was done. Group I included patients with primary single-head pterygium, most undergoing pterygium excision with conjunctival autograft (CAG). CTG-P (Conjunctival tissue graft from pterygium), AMG (Amniotic membrane graft), and inferior CAG were done in the remaining patients in this group in which conventional conjunctival autograft was a relative contraindication. Group II included patients with primary double-head pterygium who underwent vertical/horizontal split CAG, with/without limbal orientation, Inferior + Superior CAG, CTG-P, and CAG + CTG-P. Group III included patients with recurrent single-head pterygium who underwent ER (Extended resection) + LCAG (Limbal conjunctival autograft), LCAG + MMC (Mitomycin-C), CAG + MMC (Mitomycin-C) and CAG. Group IV included patients with recurrent double-head pterygium who underwent split LCAG and CAG + SLET. Results: All the four groups reported a low incidence of pterygium recurrence. Recurrence was observed at a rate of 0.47%, 3.63%, 2.86%, and 7.69% in Group I, Group II, Group III and Group IV respectively. Discussion: We mainly aimed to get minimal recurrence and good cosmetic outcomes. In double-head pterygium, we could achieve good and comparable outcomes with horizontal or vertical split CAG, with or without maintaining limbal orientation. Similarly, Inferior + Superior CAG, CTG-P, CAG+CTG-P, and AMG also showed low recurrence rates. In recurrent pterygium, ER + LCAG/CAG, with/without adjuncts like MMC showed low recurrence rates. Thus, all of these methods were found to be viable options. The main strength of our study, compared to previous studies on pterygium was its large sample size and long duration of follow-up. Conclusion: All the methods we studied had a low recurrence rate. We have formulated a treatment algorithm for pterygium management based on our outcomes. Abbreviations: CAG = Conjunctival autograft, CTG-P = Conjunctival tissue graft from pterygium, ER = Extended resection, MMC = Mitomycin-C.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
