Rasidah Alias, Yi Ling Neo, Liyun Wang, Long Zhen Sie, Hwee Jin Goh, Mohamed Yazid Mohamed Hussein, Hasnah Abdullah, Yoke Ping Wong
{"title":"Fulfilling last wishes: improving the compassionate discharge process.","authors":"Rasidah Alias, Yi Ling Neo, Liyun Wang, Long Zhen Sie, Hwee Jin Goh, Mohamed Yazid Mohamed Hussein, Hasnah Abdullah, Yoke Ping Wong","doi":"10.1136/bmjoq-2023-002666","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Compassionate discharges (ComD), commonly known as rapid discharges, are urgent one-way discharges for critically ill hospitalised patients with death expected within hours or less than 7 days, to die at their place of choice-usually in their own home. Challenges abound in this time-sensitive setting when multiple parties must work together to prepare medically unstable patients for discharge, yet healthcare staff are largely unaware of the process, resulting in delays.</p><p><strong>Methods: </strong>Process mapping, an Ishikawa diagram and a Pareto chart were used to identify barriers, which included timely acquisition of home equipment and medication and poor communication among stakeholders. In May 2020, the Quality Improvement (QI) team embarked on a pilot project to reduce family caregiver anxiety and delays in the ComD process while maintaining a success rate above 90% over a 12-month period.</p><p><strong>Interventions: </strong>Three Plan-Do-Study-Act (PDSA) cycles were used to refine a ComD resource package that was developed; this consisted of a checklist, a kit and caregiver resources. This was to support nurses, doctors and families during this difficult and emotional transition. Items in the ComD resource package were revised iteratively based on user feedback, with further data collected to measure its usefulness.</p><p><strong>Results: </strong>The 12-month ComD success rate over 3 PDSA cycles were 88.9%, 94.2% and 96.7%, respectively, after each cycle. There was a consistent reduction in the level of family anxiety before and after caregiver training and resources. Reasons for failed ComD included acute clinical deterioration or delays in obtaining home oxygen support.</p><p><strong>Conclusion: </strong>The ComD resource package allowed collaborative work across different disciplines, strengthening the safety and utility of ComD and allowing patients to die in their place of choice. These are ubiquitous across settings; this QI problem is thus relevant beyond our local institution.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"13 3","pages":""},"PeriodicalIF":2.1000,"publicationDate":"2024-07-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11253726/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2023-002666","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Compassionate discharges (ComD), commonly known as rapid discharges, are urgent one-way discharges for critically ill hospitalised patients with death expected within hours or less than 7 days, to die at their place of choice-usually in their own home. Challenges abound in this time-sensitive setting when multiple parties must work together to prepare medically unstable patients for discharge, yet healthcare staff are largely unaware of the process, resulting in delays.
Methods: Process mapping, an Ishikawa diagram and a Pareto chart were used to identify barriers, which included timely acquisition of home equipment and medication and poor communication among stakeholders. In May 2020, the Quality Improvement (QI) team embarked on a pilot project to reduce family caregiver anxiety and delays in the ComD process while maintaining a success rate above 90% over a 12-month period.
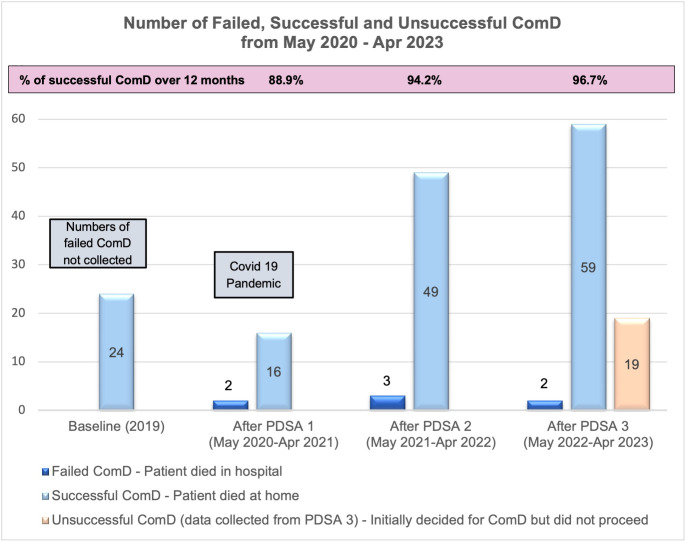
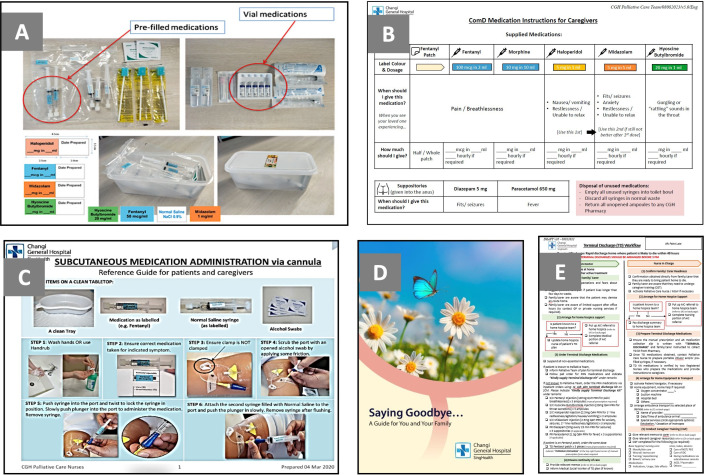
Interventions: Three Plan-Do-Study-Act (PDSA) cycles were used to refine a ComD resource package that was developed; this consisted of a checklist, a kit and caregiver resources. This was to support nurses, doctors and families during this difficult and emotional transition. Items in the ComD resource package were revised iteratively based on user feedback, with further data collected to measure its usefulness.
Results: The 12-month ComD success rate over 3 PDSA cycles were 88.9%, 94.2% and 96.7%, respectively, after each cycle. There was a consistent reduction in the level of family anxiety before and after caregiver training and resources. Reasons for failed ComD included acute clinical deterioration or delays in obtaining home oxygen support.
Conclusion: The ComD resource package allowed collaborative work across different disciplines, strengthening the safety and utility of ComD and allowing patients to die in their place of choice. These are ubiquitous across settings; this QI problem is thus relevant beyond our local institution.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
