{"title":"Percutaneous Endovascular Creation of a Neo-arteriovenous Fistula in Dysfunctional Hemodialysis Fistulas.","authors":"Huei-Lung Liang, Ming-Feng Li, Chia-Ling Chiang","doi":"10.1007/s00270-024-03804-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Arteriovenous fistulas (AVF) is the preferred type of hemodialysis access, but when an arteriovenous anastomosis (AVA) calcifies, surgical revision of the AVF may be required. We report a technique to create percutaneous artery-to-vein intervascular neo-fistulas for re-anastomosis of AVA and evaluate its safety and efficacy.</p><p><strong>Materials and methods: </strong>9 patients who failed either guidewire navigation or conventional balloon dilation for calcified AVA stenosis/occlusion underwent a salvage procedure of their dialysis shunt by the percutaneous creation of a new arteriovenous fistula. Needle puncture of the adjacent supplying artery and outflow vein under ultrasonographic and/or fluoroscopic guidance was performed and followed by balloon dilation, with or without stent graft placement. The detailed techniques, technical success, primary neo-fistula patency, primary and secondary access patency rates were reported herein.</p><p><strong>Results: </strong>Technical success was achieved in 100% of the 9 patients treated (7 neo-fistulas with stents and 2 neo-fistulas without stent placement). The median primary neo-fistula and access patencies were 15 and 5 months, respectively. The primary neo-fistula patency rates at 6, 12, and 18 months were 72.9%, 54.7% and 27.9%, respectively, with secondary neo-fistula and access patency rates of 72.9%, 72.9% and 72.9%, respectively. One delayed complication of pseudoaneurysm formation occurred, which was managed by the successful endovascular deployment of a stent graft on an out-patient basis.</p><p><strong>Conclusion: </strong>Percutaneous artery-to-vein intervascular neo-fistula creation is feasible for re-anastomosing calcified AVA, with low adverse effects and acceptable primary neo-fistula and secondary access patency.</p>","PeriodicalId":9591,"journal":{"name":"CardioVascular and Interventional Radiology","volume":" ","pages":"1142-1147"},"PeriodicalIF":2.9000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CardioVascular and Interventional Radiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00270-024-03804-y","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/15 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: Arteriovenous fistulas (AVF) is the preferred type of hemodialysis access, but when an arteriovenous anastomosis (AVA) calcifies, surgical revision of the AVF may be required. We report a technique to create percutaneous artery-to-vein intervascular neo-fistulas for re-anastomosis of AVA and evaluate its safety and efficacy.
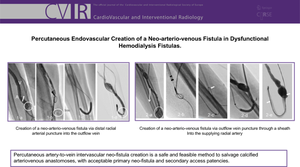
Materials and methods: 9 patients who failed either guidewire navigation or conventional balloon dilation for calcified AVA stenosis/occlusion underwent a salvage procedure of their dialysis shunt by the percutaneous creation of a new arteriovenous fistula. Needle puncture of the adjacent supplying artery and outflow vein under ultrasonographic and/or fluoroscopic guidance was performed and followed by balloon dilation, with or without stent graft placement. The detailed techniques, technical success, primary neo-fistula patency, primary and secondary access patency rates were reported herein.
Results: Technical success was achieved in 100% of the 9 patients treated (7 neo-fistulas with stents and 2 neo-fistulas without stent placement). The median primary neo-fistula and access patencies were 15 and 5 months, respectively. The primary neo-fistula patency rates at 6, 12, and 18 months were 72.9%, 54.7% and 27.9%, respectively, with secondary neo-fistula and access patency rates of 72.9%, 72.9% and 72.9%, respectively. One delayed complication of pseudoaneurysm formation occurred, which was managed by the successful endovascular deployment of a stent graft on an out-patient basis.
Conclusion: Percutaneous artery-to-vein intervascular neo-fistula creation is feasible for re-anastomosing calcified AVA, with low adverse effects and acceptable primary neo-fistula and secondary access patency.
期刊介绍:
CardioVascular and Interventional Radiology (CVIR) is the official journal of the Cardiovascular and Interventional Radiological Society of Europe, and is also the official organ of a number of additional distinguished national and international interventional radiological societies. CVIR publishes double blinded peer-reviewed original research work including clinical and laboratory investigations, technical notes, case reports, works in progress, and letters to the editor, as well as review articles, pictorial essays, editorials, and special invited submissions in the field of vascular and interventional radiology. Beside the communication of the latest research results in this field, it is also the aim of CVIR to support continuous medical education. Articles that are accepted for publication are done so with the understanding that they, or their substantive contents, have not been and will not be submitted to any other publication.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
