{"title":"Real-world use and outcomes of targeted therapy and immunotherapy for adjuvant treatment of BRAF -mutated melanoma patients in the United States.","authors":"Sanjay Chandrasekaran, You-Li Ling, Jackson Tang","doi":"10.1097/CMR.0000000000000990","DOIUrl":null,"url":null,"abstract":"<p><p>Using a customized, harmonized US electronic health record database, real-world prescription patterns of first-line adjuvant immunotherapy and targeted therapy were retrospectively assessed for BRAF V600-mutated melanoma. Adults with BRAF V600 mutation-positive stage IIIA-D cutaneous melanoma who received first-line adjuvant immunotherapy (nivolumab or pembrolizumab) or targeted therapy (dabrafenib plus trametinib) between 1 January 2014 and 30 August 2020 in the NOBLE database were included. Patients were followed from first-line adjuvant therapy initiation for at least 6 months, until death, progression, follow-up loss, or data cutoff. Primary endpoints were proportion of patients receiving either therapy in first-line and second-line, treatment switching, treatment timing, and status at the end of first-line therapy. Secondary endpoints included discontinuation rates, recurrence-free survival (RFS), and overall survival (OS). Of 318 patients evaluated, 67.6% received nivolumab, 14.2% pembrolizumab, and 18.2% targeted therapy as first-line adjuvant therapy. Median treatment duration was longest for nivolumab (292 days) and shortest for targeted therapy (115 days). Reason for discontinuation was recorded for 195 of 274 patients who discontinued first-line therapy; most common reasons were treatment completion and treatment-related toxicity [87/158 (55.0%) and 29/158 (18.4%), respectively, in immunotherapy-treated patients; 9/37 (24.3%) and 21/37 (56.8%) in targeted therapy-treated patients]. Median RFS and OS for targeted therapy and nivolumab were not reached and were 34.6 and 38.1 months, respectively, for pembrolizumab. These results inform on prescription preferences and clinical outcomes for BRAF V600-mutated melanoma patients in the first-line adjuvant setting.</p>","PeriodicalId":18550,"journal":{"name":"Melanoma Research","volume":" ","pages":"457-464"},"PeriodicalIF":1.9000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11361351/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Melanoma Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/CMR.0000000000000990","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/16 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"DERMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
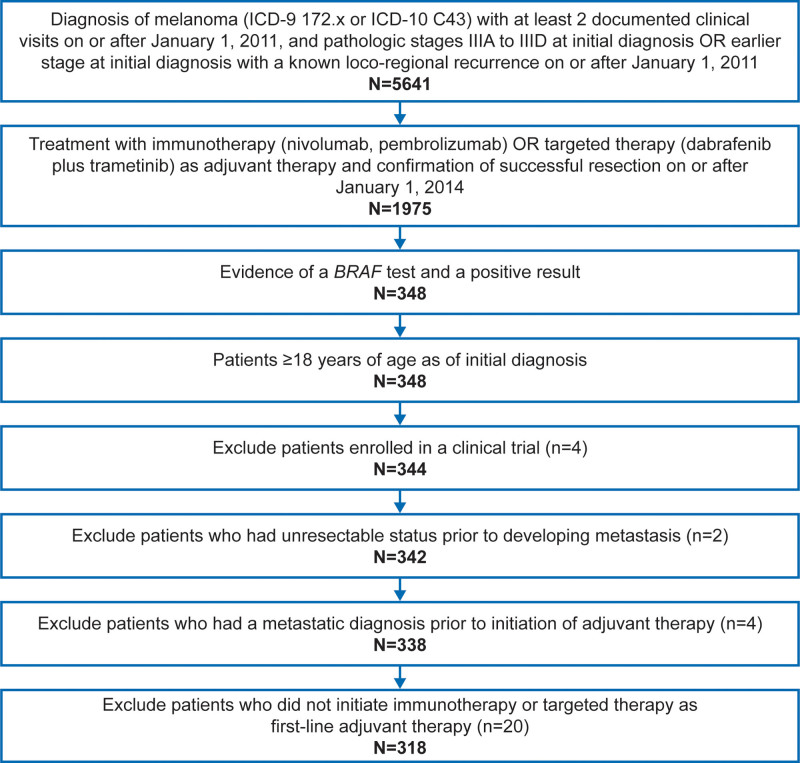
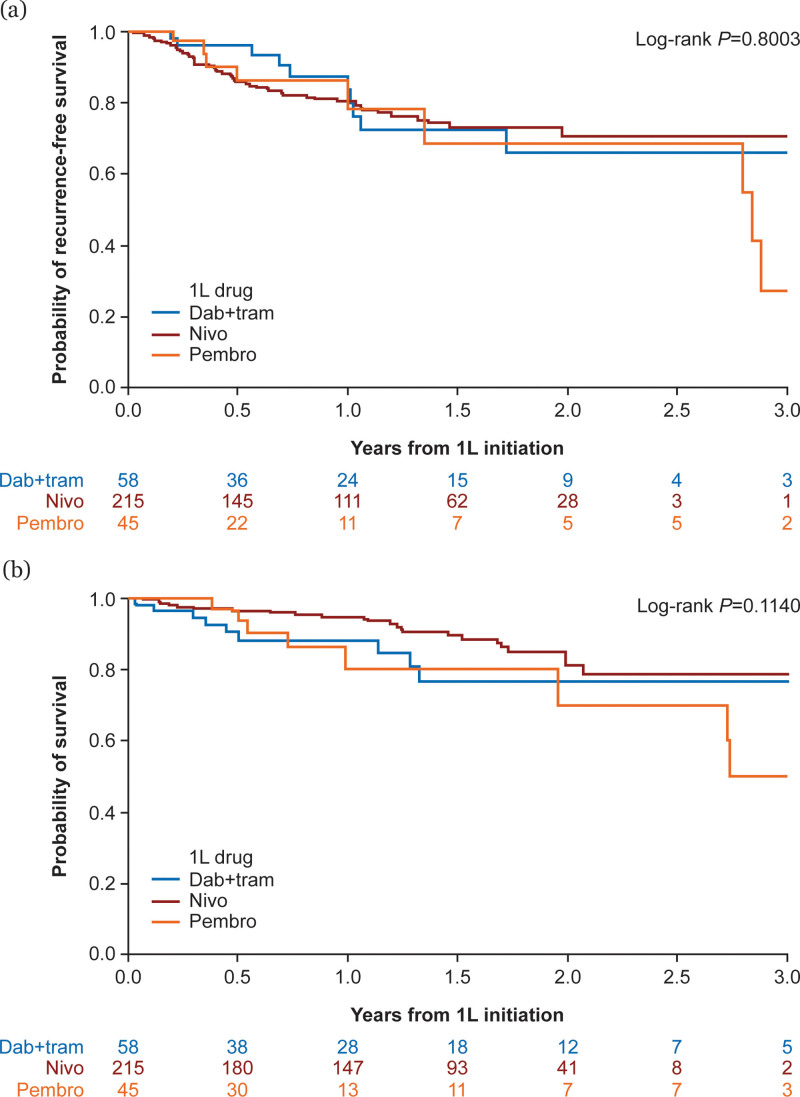
Using a customized, harmonized US electronic health record database, real-world prescription patterns of first-line adjuvant immunotherapy and targeted therapy were retrospectively assessed for BRAF V600-mutated melanoma. Adults with BRAF V600 mutation-positive stage IIIA-D cutaneous melanoma who received first-line adjuvant immunotherapy (nivolumab or pembrolizumab) or targeted therapy (dabrafenib plus trametinib) between 1 January 2014 and 30 August 2020 in the NOBLE database were included. Patients were followed from first-line adjuvant therapy initiation for at least 6 months, until death, progression, follow-up loss, or data cutoff. Primary endpoints were proportion of patients receiving either therapy in first-line and second-line, treatment switching, treatment timing, and status at the end of first-line therapy. Secondary endpoints included discontinuation rates, recurrence-free survival (RFS), and overall survival (OS). Of 318 patients evaluated, 67.6% received nivolumab, 14.2% pembrolizumab, and 18.2% targeted therapy as first-line adjuvant therapy. Median treatment duration was longest for nivolumab (292 days) and shortest for targeted therapy (115 days). Reason for discontinuation was recorded for 195 of 274 patients who discontinued first-line therapy; most common reasons were treatment completion and treatment-related toxicity [87/158 (55.0%) and 29/158 (18.4%), respectively, in immunotherapy-treated patients; 9/37 (24.3%) and 21/37 (56.8%) in targeted therapy-treated patients]. Median RFS and OS for targeted therapy and nivolumab were not reached and were 34.6 and 38.1 months, respectively, for pembrolizumab. These results inform on prescription preferences and clinical outcomes for BRAF V600-mutated melanoma patients in the first-line adjuvant setting.
期刊介绍:
Melanoma Research is a well established international forum for the dissemination of new findings relating to melanoma. The aim of the Journal is to promote the level of informational exchange between those engaged in the field. Melanoma Research aims to encourage an informed and balanced view of experimental and clinical research and extend and stimulate communication and exchange of knowledge between investigators with differing areas of expertise. This will foster the development of translational research. The reporting of new clinical results and the effect and toxicity of new therapeutic agents and immunotherapy will be given emphasis by rapid publication of Short Communications. Thus, Melanoma Research seeks to present a coherent and up-to-date account of all aspects of investigations pertinent to melanoma. Consequently the scope of the Journal is broad, embracing the entire range of studies from fundamental and applied research in such subject areas as genetics, molecular biology, biochemistry, cell biology, photobiology, pathology, immunology, and advances in clinical oncology influencing the prevention, diagnosis and treatment of melanoma.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
