Huijie Yu, Xudong Ma, Meijun Pang, Xuehai Fan, Yan Xing, Kuo Zhang, Ningnannan Zhang, Cai Li, Kai Yu, Xiuyun Liu
{"title":"A female patient with Alzheimer's disease via multimodality diagnostic approaches: A case report","authors":"Huijie Yu, Xudong Ma, Meijun Pang, Xuehai Fan, Yan Xing, Kuo Zhang, Ningnannan Zhang, Cai Li, Kai Yu, Xiuyun Liu","doi":"10.1002/brx2.69","DOIUrl":null,"url":null,"abstract":"<p>Alzheimer's disease (AD) is a neurodegenerative disease and the most common cause of dementia, accounting for around 60%–70% dementia cases.<span><sup>1</sup></span> Normal pressure hydrocephalus (NPH) is one of the few reversible causes of dementia, accounting for approximately 6% of all dementias, among which, idiopathic normal pressure hydrocephalus (iNPH) happens mostly in elder people.<span><sup>2</sup></span> Due to the similarity of their symptoms, it is important to differentiate between iNPH and AD.<span><sup>3</sup></span> In this paper, we reported a case who were originally diagnosed with iNPH and were finally found to be an AD patient via multimodality diagnostic approaches.</p><p>A 57-year-old woman, who got a short-term memory decline 2 years ago, was admitted to Tianjin Medical University General Hospital (Tianjin, China) in October 2023. Her speech, numeracy, and social networking ability also declined. She went to a local hospital 2 years ago and was diagnosed with iNPH. She was admitted to our hospital as a result of her symptoms progressively getting worse over the past few months and her gait deteriorating. The doctors suspected her as an iNPH or AD patient, thus arranging magnetic resonance imaging (MRI), cerebrospinal fluid tap test (CSF TT), Infusion study, phase-contrast magnetic resonance imaging (PC-MRI) on the admission day.</p><p>As shown in Figure 1, the MRI showed significant ventricular dilation, with an Evans index (EI) of 0.38. However, her Callosal Angle was 90.6°, and presented a negative DESH sign (disproportionately enlarged subarachnoid space hydrocephalus). Obvious atrophies were found in temporal lobe and parahippocampal gyrus. The PC-MRI shows enhanced cerebrospinal fluid flow signals in the ventricular system, with thinning of cerebral white matter. The imaging manifestations didn't quite match the main features of iNPH, she looks more like a dementia or an AD patient.</p><p>The CSF TT is a clinical tool for the diagnosis of iNPH, and has been regarded as an important prediction tool of shunt effectiveness in patients with suspected iNPH.<span><sup>4</sup></span> During CSF TT, 30–50 mL CSF was released through a lumbar puncture, and patient's gait balance ability, bladder function, cognitive function was evaluated before and 24/48/72 h after CSF TT. No significant improvement was found after the CSF TT test.</p><p>Infusion study has been a well-defined method to assess the necessity of proceeding into shunt for iNPH patients. It offers several advantages and alternatives compared to traditional CSF TT, including short-testing duration, calculation of resistance to CSF outflow (Rout) and elasticity.<span><sup>5</sup></span> For this patient, the infusion study showed an opening pressure of 9 mmHg, and resistance of CSF was 3.53 mmHg × min/mL, which indicates smooth CSF circulation (Supporting Information S1).</p><p>The patient declared slight alleviation after the CSF TT, however, the clinical assessment by doctors didn't show obvious improvement. Thus, we recommended her to do a positron emission tomography/computed tomography (PET/CT) imaging test. Figure 1D showed an accumulation of Amyloid beta (Aβ) protein, a well-known indicator of AD disease, which has facilitated doctors to accurately pre-diagnose cases of AD. Finally, via multimodality diagnostic approaches, we confirmed that she has AD.</p><p>Both AD and iNPH can cause dementia, exhibiting significant similarities and symptoms, such as cognitive decline, neurodegeneration, physical deterioration, and sleep disorders. But symptoms appear at different order. In iNPH, physical impairments, especially in walking and urinary continence, are the first to decline. By contrast, cognitive decline tends to be an early feature in AD. While AD is an irreversible neurodegenerative disease, symptoms caused by iNPH can be reversed by ventriculoperitoneal shunt. Therefore, it is important for clinicians to distinguish between them to avoid delays in diagnosis and waste of healthcare resources. The multimodality diagnostic approaches allows doctors identify diseases by considering multiple indicators, minimize the risk of misdiagnosis. A wider perspective gained through interdisciplinary collaboration may yield novel insights and facilitate earlier diagnosis.</p><p>This is one case started with cognitive impairment and has the classic indicators of iNPH, including impaired cognition, gait, and elevated EI. The patient was incorrectly diagnosed with iNPH at the local hospital, resulting in a delay in the disease treatment and a waste of healthcare resources. At our hospital, based on multimodality diagnostic approaches, including MRI, PC-MRI, Infusion study, CSF TT and PET/CT, we make individually and precisely diagnosis for the patient.</p><p><b>Huijie Yu</b>: Conceptualization; investigation; supervision; writing – original draft. <b>Xudong Ma</b>: Data curation; formal analysis; investigation; writing – original draft; writing – review & editing. <b>Meijun Pang</b>: Formal analysis; writing – review & editing. <b>Xuehai Fan</b>: Data curation; writing – review & editing. <b>Yan Xing</b>: Investigation; writing – review & editing. <b>Kuo Zhang</b>: Formal analysis; writing – review & editing. <b>Ningnannan Zhang</b>: Data curation; investigation; writing – review & editing. <b>Cai Li</b>: Data curation; writing – review & editing. <b>Kai Yu</b>: Conceptualization; investigation; writing – review & editing. <b>Xiuyun Liu</b>: Investigation; supervision; writing – review & editing.</p><p>The authors declare no conflicts of interest.</p><p>The study was approved by Ethics Committee of Tianjin Medical University General Hospital (IRB2024-YX-171-01). The patient signed the consent form and agreed to participate in this study.</p>","PeriodicalId":94303,"journal":{"name":"Brain-X","volume":"2 3","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2024-07-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/brx2.69","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Brain-X","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/brx2.69","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Alzheimer's disease (AD) is a neurodegenerative disease and the most common cause of dementia, accounting for around 60%–70% dementia cases.1 Normal pressure hydrocephalus (NPH) is one of the few reversible causes of dementia, accounting for approximately 6% of all dementias, among which, idiopathic normal pressure hydrocephalus (iNPH) happens mostly in elder people.2 Due to the similarity of their symptoms, it is important to differentiate between iNPH and AD.3 In this paper, we reported a case who were originally diagnosed with iNPH and were finally found to be an AD patient via multimodality diagnostic approaches.
A 57-year-old woman, who got a short-term memory decline 2 years ago, was admitted to Tianjin Medical University General Hospital (Tianjin, China) in October 2023. Her speech, numeracy, and social networking ability also declined. She went to a local hospital 2 years ago and was diagnosed with iNPH. She was admitted to our hospital as a result of her symptoms progressively getting worse over the past few months and her gait deteriorating. The doctors suspected her as an iNPH or AD patient, thus arranging magnetic resonance imaging (MRI), cerebrospinal fluid tap test (CSF TT), Infusion study, phase-contrast magnetic resonance imaging (PC-MRI) on the admission day.
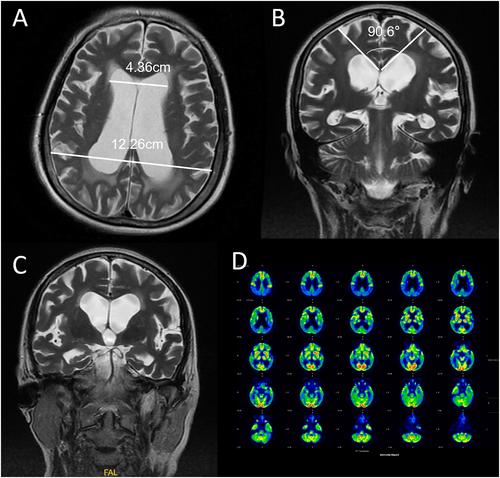
As shown in Figure 1, the MRI showed significant ventricular dilation, with an Evans index (EI) of 0.38. However, her Callosal Angle was 90.6°, and presented a negative DESH sign (disproportionately enlarged subarachnoid space hydrocephalus). Obvious atrophies were found in temporal lobe and parahippocampal gyrus. The PC-MRI shows enhanced cerebrospinal fluid flow signals in the ventricular system, with thinning of cerebral white matter. The imaging manifestations didn't quite match the main features of iNPH, she looks more like a dementia or an AD patient.
The CSF TT is a clinical tool for the diagnosis of iNPH, and has been regarded as an important prediction tool of shunt effectiveness in patients with suspected iNPH.4 During CSF TT, 30–50 mL CSF was released through a lumbar puncture, and patient's gait balance ability, bladder function, cognitive function was evaluated before and 24/48/72 h after CSF TT. No significant improvement was found after the CSF TT test.
Infusion study has been a well-defined method to assess the necessity of proceeding into shunt for iNPH patients. It offers several advantages and alternatives compared to traditional CSF TT, including short-testing duration, calculation of resistance to CSF outflow (Rout) and elasticity.5 For this patient, the infusion study showed an opening pressure of 9 mmHg, and resistance of CSF was 3.53 mmHg × min/mL, which indicates smooth CSF circulation (Supporting Information S1).
The patient declared slight alleviation after the CSF TT, however, the clinical assessment by doctors didn't show obvious improvement. Thus, we recommended her to do a positron emission tomography/computed tomography (PET/CT) imaging test. Figure 1D showed an accumulation of Amyloid beta (Aβ) protein, a well-known indicator of AD disease, which has facilitated doctors to accurately pre-diagnose cases of AD. Finally, via multimodality diagnostic approaches, we confirmed that she has AD.
Both AD and iNPH can cause dementia, exhibiting significant similarities and symptoms, such as cognitive decline, neurodegeneration, physical deterioration, and sleep disorders. But symptoms appear at different order. In iNPH, physical impairments, especially in walking and urinary continence, are the first to decline. By contrast, cognitive decline tends to be an early feature in AD. While AD is an irreversible neurodegenerative disease, symptoms caused by iNPH can be reversed by ventriculoperitoneal shunt. Therefore, it is important for clinicians to distinguish between them to avoid delays in diagnosis and waste of healthcare resources. The multimodality diagnostic approaches allows doctors identify diseases by considering multiple indicators, minimize the risk of misdiagnosis. A wider perspective gained through interdisciplinary collaboration may yield novel insights and facilitate earlier diagnosis.
This is one case started with cognitive impairment and has the classic indicators of iNPH, including impaired cognition, gait, and elevated EI. The patient was incorrectly diagnosed with iNPH at the local hospital, resulting in a delay in the disease treatment and a waste of healthcare resources. At our hospital, based on multimodality diagnostic approaches, including MRI, PC-MRI, Infusion study, CSF TT and PET/CT, we make individually and precisely diagnosis for the patient.
Huijie Yu: Conceptualization; investigation; supervision; writing – original draft. Xudong Ma: Data curation; formal analysis; investigation; writing – original draft; writing – review & editing. Meijun Pang: Formal analysis; writing – review & editing. Xuehai Fan: Data curation; writing – review & editing. Yan Xing: Investigation; writing – review & editing. Kuo Zhang: Formal analysis; writing – review & editing. Ningnannan Zhang: Data curation; investigation; writing – review & editing. Cai Li: Data curation; writing – review & editing. Kai Yu: Conceptualization; investigation; writing – review & editing. Xiuyun Liu: Investigation; supervision; writing – review & editing.
The authors declare no conflicts of interest.
The study was approved by Ethics Committee of Tianjin Medical University General Hospital (IRB2024-YX-171-01). The patient signed the consent form and agreed to participate in this study.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
