Longitudinal cohort study of discrepancies between prescribed and administered polypharmacy rates: implications for National Aged Care Quality Indicator Programs.
Nasir Wabe, Rachel Urwin, Karla Seaman, Johanna I Westbrook
{"title":"Longitudinal cohort study of discrepancies between prescribed and administered polypharmacy rates: implications for National Aged Care Quality Indicator Programs.","authors":"Nasir Wabe, Rachel Urwin, Karla Seaman, Johanna I Westbrook","doi":"10.1136/bmjqs-2023-017042","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Polypharmacy is frequently used as a quality indicator for older adults in Residential Aged Care Facilities (RACFs) and is measured using a range of definitions. The impact of data source choice on polypharmacy rates and the implications for monitoring and benchmarking remain unclear. We aimed to determine polypharmacy rates (≥9 concurrent medicines) by using prescribed and administered data under various scenarios, leveraging electronic data from 30 RACFs.</p><p><strong>Method: </strong>A longitudinal cohort study of 5662 residents in New South Wales, Australia. Both prescribed and administered polypharmacy rates were calculated biweekly from January 2019 to September 2022, providing 156 assessment times. 12 different polypharmacy rates were computed separately using prescribing and administration data and incorporating different combinations of items: <i>medicines and non-medicinal products</i>, <i>any medicines</i> and <i>regular medicines</i> across four scenarios: no, 1-week, 2-week and 4-week look-back periods. Generalised estimating equation models were employed to identify predictors of discrepancies between prescribed and administered polypharmacy.</p><p><strong>Results: </strong>Polypharmacy rates among residents ranged from 33.9% using data on administered <i>regular medicines</i> with no look-back period to 63.5% using prescribed <i>medicines and non-medicinal products</i> with a 4-week look-back period. At each assessment time, the differences between prescribed and administered polypharmacy rates were consistently more than 10.0%, 4.5%, 3.5% and 3.0%, respectively, with no, 1-week, 2-week and 4-week look-back periods. Diabetic residents faced over two times the likelihood of polypharmacy discrepancies compared with counterparts, while dementia residents consistently showed reduced likelihood across all analyses.</p><p><strong>Conclusion: </strong>We found notable discrepancies between polypharmacy rates for prescribed and administered medicines. We recommend a review of the guidance for calculating and interpreting polypharmacy for national quality indicator programmes to ensure consistent measurement and meaningful reporting.</p>","PeriodicalId":9077,"journal":{"name":"BMJ Quality & Safety","volume":" ","pages":"780-789"},"PeriodicalIF":6.5000,"publicationDate":"2024-11-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11671870/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Quality & Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/bmjqs-2023-017042","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Polypharmacy is frequently used as a quality indicator for older adults in Residential Aged Care Facilities (RACFs) and is measured using a range of definitions. The impact of data source choice on polypharmacy rates and the implications for monitoring and benchmarking remain unclear. We aimed to determine polypharmacy rates (≥9 concurrent medicines) by using prescribed and administered data under various scenarios, leveraging electronic data from 30 RACFs.
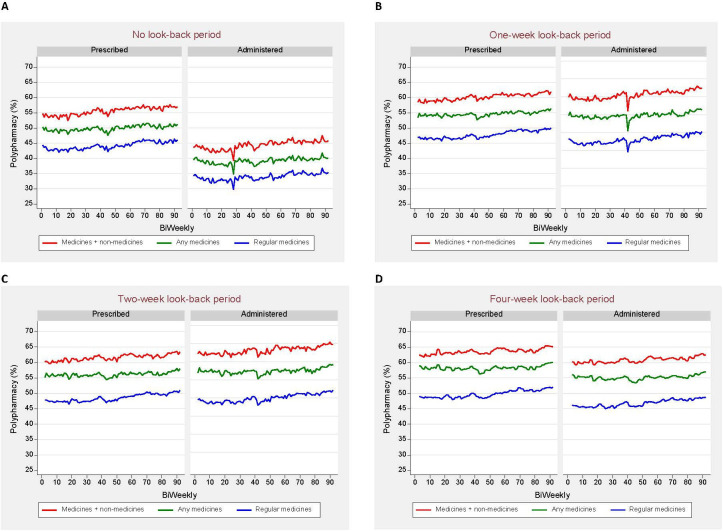
Method: A longitudinal cohort study of 5662 residents in New South Wales, Australia. Both prescribed and administered polypharmacy rates were calculated biweekly from January 2019 to September 2022, providing 156 assessment times. 12 different polypharmacy rates were computed separately using prescribing and administration data and incorporating different combinations of items: medicines and non-medicinal products, any medicines and regular medicines across four scenarios: no, 1-week, 2-week and 4-week look-back periods. Generalised estimating equation models were employed to identify predictors of discrepancies between prescribed and administered polypharmacy.
Results: Polypharmacy rates among residents ranged from 33.9% using data on administered regular medicines with no look-back period to 63.5% using prescribed medicines and non-medicinal products with a 4-week look-back period. At each assessment time, the differences between prescribed and administered polypharmacy rates were consistently more than 10.0%, 4.5%, 3.5% and 3.0%, respectively, with no, 1-week, 2-week and 4-week look-back periods. Diabetic residents faced over two times the likelihood of polypharmacy discrepancies compared with counterparts, while dementia residents consistently showed reduced likelihood across all analyses.
Conclusion: We found notable discrepancies between polypharmacy rates for prescribed and administered medicines. We recommend a review of the guidance for calculating and interpreting polypharmacy for national quality indicator programmes to ensure consistent measurement and meaningful reporting.
期刊介绍:
BMJ Quality & Safety (previously Quality & Safety in Health Care) is an international peer review publication providing research, opinions, debates and reviews for academics, clinicians and healthcare managers focused on the quality and safety of health care and the science of improvement.
The journal receives approximately 1000 manuscripts a year and has an acceptance rate for original research of 12%. Time from submission to first decision averages 22 days and accepted articles are typically published online within 20 days. Its current impact factor is 3.281.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
