{"title":"Unilateral Anterior Spinal Artery Syndrome following Spinal Anesthesia for Cesarian Section: A Case Report.","authors":"Matthew J Kraus, Joseph Nguyen","doi":"10.1159/000539405","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Spinal cord infarction is a rare but serious neurologic complication of spinal anesthesia. Direct vessel injury, intra-arterial anesthetic injection, and anesthetic-induced local hypotension are potential mechanisms of infarction during this procedure. The proximity of the artery of Adamkiewicz to the spinal levels used for spinal anesthesia may also play a role. This case of unilateral anterior spinal artery syndrome highlights the potential for an atypical pattern of injury and deficits due to the complexity of the spinal cord's anterior circulation.</p><p><strong>Case presentation: </strong>We present a 38-year-old female patient who presented with left lower extremity weakness, loss of temperature sensation, and urinary retention following spinal anesthesia for cesarian section. Magnetic resonance imaging of the spine demonstrated T2 hyperintensities in the left central spinal cord from T8 to the conus medullaris. A diagnosis of spinal cord infarction was made after lumbar puncture testing showed no evidence of inflammatory myelitis. The patient was treated with steroids empirically until lumbar puncture testing showed no inflammation. The patient was discharged on daily aspirin with persistent left lower extremity weakness and loss of temperature sensation. A plan for outpatient physical therapy was made for rehabilitation.</p><p><strong>Conclusion: </strong>Awareness of the potential for spinal cord infarction secondary to spinal anesthesia must increase among anesthesiologists, obstetricians, and neurologists. The risk of systemic hypotension during and after spinal anesthesia is important to recognize for both primary and secondary prevention of this complication. The hyperacute onset of myelopathic symptoms should point neurologists to investigate an ischemic etiology in the proper clinical context.</p>","PeriodicalId":9639,"journal":{"name":"Case Reports in Neurology","volume":"16 1","pages":"142-147"},"PeriodicalIF":0.6000,"publicationDate":"2024-05-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11250075/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Neurology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000539405","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Spinal cord infarction is a rare but serious neurologic complication of spinal anesthesia. Direct vessel injury, intra-arterial anesthetic injection, and anesthetic-induced local hypotension are potential mechanisms of infarction during this procedure. The proximity of the artery of Adamkiewicz to the spinal levels used for spinal anesthesia may also play a role. This case of unilateral anterior spinal artery syndrome highlights the potential for an atypical pattern of injury and deficits due to the complexity of the spinal cord's anterior circulation.
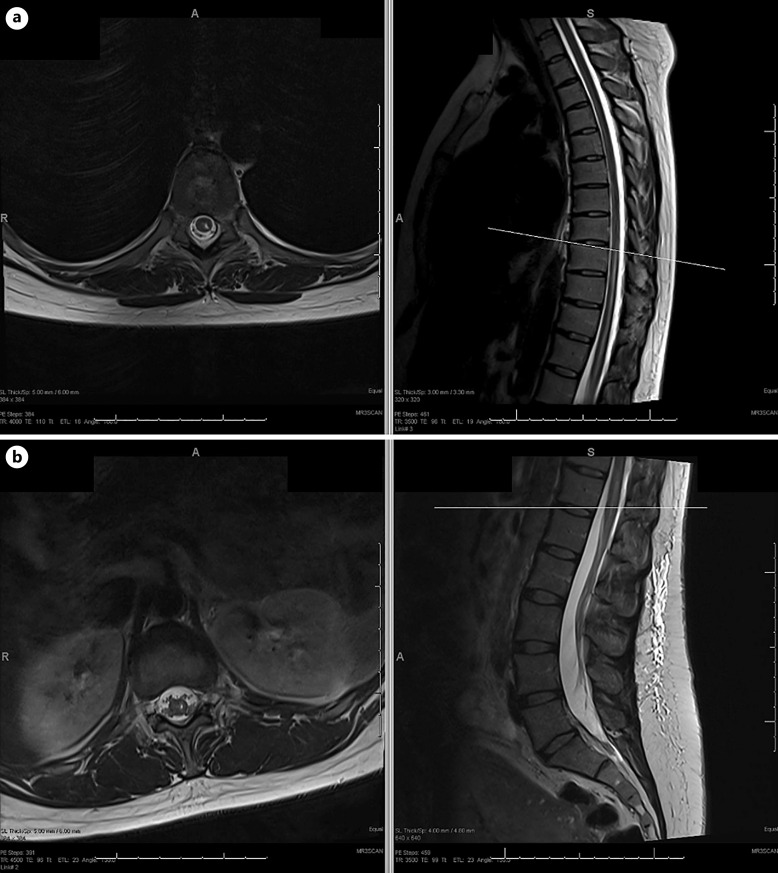
Case presentation: We present a 38-year-old female patient who presented with left lower extremity weakness, loss of temperature sensation, and urinary retention following spinal anesthesia for cesarian section. Magnetic resonance imaging of the spine demonstrated T2 hyperintensities in the left central spinal cord from T8 to the conus medullaris. A diagnosis of spinal cord infarction was made after lumbar puncture testing showed no evidence of inflammatory myelitis. The patient was treated with steroids empirically until lumbar puncture testing showed no inflammation. The patient was discharged on daily aspirin with persistent left lower extremity weakness and loss of temperature sensation. A plan for outpatient physical therapy was made for rehabilitation.
Conclusion: Awareness of the potential for spinal cord infarction secondary to spinal anesthesia must increase among anesthesiologists, obstetricians, and neurologists. The risk of systemic hypotension during and after spinal anesthesia is important to recognize for both primary and secondary prevention of this complication. The hyperacute onset of myelopathic symptoms should point neurologists to investigate an ischemic etiology in the proper clinical context.
期刊介绍:
This new peer-reviewed online-only journal publishes original case reports covering the entire spectrum of neurology. Clinicians and researchers are given a tool to disseminate their personal experience to a wider public as well as to review interesting cases encountered by colleagues all over the world. To complement the contributions supplementary material is welcomed. The reports are searchable according to the key words supplied by the authors; it will thus be possible to search across the entire growing collection of case reports with universally used terms, further facilitating the retrieval of specific information. Following the open access principle, the entire contents can be retrieved at no charge, guaranteeing easy access to this valuable source of anecdotal information at all times.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
