Outcomes in patients with out-of-hospital cardiac arrest according to prehospital advanced airway management timing: a retrospective observational study.
{"title":"Outcomes in patients with out-of-hospital cardiac arrest according to prehospital advanced airway management timing: a retrospective observational study.","authors":"Sang-Hun Lee, Hyun Wook Ryoo","doi":"10.12701/jyms.2024.00332","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with out-of-hospital cardiac arrest (OHCA), guidelines recommend advanced airway (AA) management at the advanced cardiovascular life support stage; however, the ideal timing remains controversial. Therefore, we evaluated the prognosis according to the timing of AA in patients with OHCA.</p><p><strong>Methods: </strong>We conducted a retrospective observational study of patients with OHCA at six major hospitals in Daegu Metropolitan City, South Korea, from August 2019 to June 2022. We compared groups with early and late AA and evaluated prognosis, including recovery of spontaneous circulation (ROSC), survival to discharge, and neurological evaluation, according to AA timing.</p><p><strong>Results: </strong>Of 2,087 patients with OHCA, 945 underwent early AA management and 1,142 underwent late AA management. The timing of AA management did not influence ROSC in the emergency department (5-6 minutes: adjusted odds ratio [aOR], 0.97; p=0.914; 7-9 minutes: aOR, 1.37; p=0.223; ≥10 minutes: aOR, 1.32; p=0.345). The timing of AA management also did not influence survival to discharge (5-6 minutes: aOR, 0.79; p=0.680; 7-9 minutes: aOR, 1.04; p=0.944; ≥10 minutes: aOR, 1.86; p=0.320) or good neurological outcomes (5-6 minutes: aOR, 1.72; p=0.512; 7-9 minutes: aOR, 0.48; p=0.471; ≥10 minutes: aOR, 0.96; p=0.892).</p><p><strong>Conclusion: </strong>AA timing in patients with OHCA was not associated with ROSC, survival to hospital discharge, or neurological outcomes.</p>","PeriodicalId":74020,"journal":{"name":"Journal of Yeungnam medical science","volume":" ","pages":"288-295"},"PeriodicalIF":1.4000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11534406/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Yeungnam medical science","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12701/jyms.2024.00332","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/18 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In patients with out-of-hospital cardiac arrest (OHCA), guidelines recommend advanced airway (AA) management at the advanced cardiovascular life support stage; however, the ideal timing remains controversial. Therefore, we evaluated the prognosis according to the timing of AA in patients with OHCA.
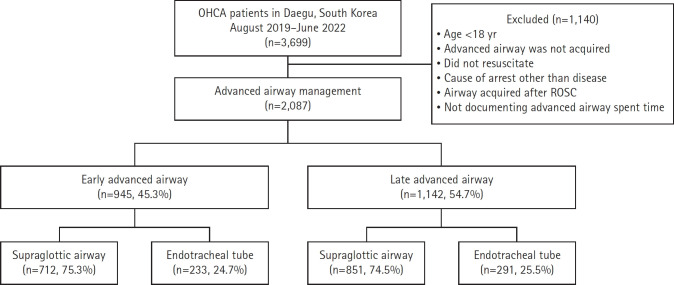
Methods: We conducted a retrospective observational study of patients with OHCA at six major hospitals in Daegu Metropolitan City, South Korea, from August 2019 to June 2022. We compared groups with early and late AA and evaluated prognosis, including recovery of spontaneous circulation (ROSC), survival to discharge, and neurological evaluation, according to AA timing.
Results: Of 2,087 patients with OHCA, 945 underwent early AA management and 1,142 underwent late AA management. The timing of AA management did not influence ROSC in the emergency department (5-6 minutes: adjusted odds ratio [aOR], 0.97; p=0.914; 7-9 minutes: aOR, 1.37; p=0.223; ≥10 minutes: aOR, 1.32; p=0.345). The timing of AA management also did not influence survival to discharge (5-6 minutes: aOR, 0.79; p=0.680; 7-9 minutes: aOR, 1.04; p=0.944; ≥10 minutes: aOR, 1.86; p=0.320) or good neurological outcomes (5-6 minutes: aOR, 1.72; p=0.512; 7-9 minutes: aOR, 0.48; p=0.471; ≥10 minutes: aOR, 0.96; p=0.892).
Conclusion: AA timing in patients with OHCA was not associated with ROSC, survival to hospital discharge, or neurological outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
