Charlotte Mund, Katharina Asmus, Wajima Safi, Oliver Ritter, Dominique Petrus, Susann Patschan, Daniel Patschan
{"title":"Clinically Evident Cardiopulmonary Congestion Does Not Significantly Impact the Prognosis of Patients With Septic Acute Kidney Injury.","authors":"Charlotte Mund, Katharina Asmus, Wajima Safi, Oliver Ritter, Dominique Petrus, Susann Patschan, Daniel Patschan","doi":"10.14740/jocmr5190","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute kidney injury (AKI) is a common issue among in-hospital patients, with high mortality rates. Sepsis is a primary cause of AKI, particularly in the intensive care unit. Patients with septic AKI often experience cardiovascular congestion, leading to the formal classification of cardiorenal syndrome type 5. The study aimed to evaluate the prognosis of septic AKI patients with and without clinical evidence of cardiovascular congestion.</p><p><strong>Methods: </strong>This was a retrospective observational study. AKI patients were identified using the in-hospital AKI alert system. Sepsis was diagnosed based on laboratory, clinical, and hemodynamic characteristics, with additional consideration of the quickSOFA score. Cardiovascular congestion was diagnosed by assessing clinical (edema), radiographic (pulmonary congestion), echocardiographic (e.g., wall motion abnormalities), and laboratory variables (e.g., N-terminal pro-B-type natriuretic peptide). Endpoints included in-hospital survival, the need for kidney replacement therapy (KRT), and recovery of kidney function (ROKF).</p><p><strong>Results: </strong>In total, 102 patients were included, and cardiopulmonary congestion was diagnosed in 78.4%. Individuals with congestion did not differ from patients without congestion in any of the pre-defined endpoints.</p><p><strong>Conclusions: </strong>It is justified not to consider clinically apparent cardiovascular congestion in septic AKI patients as a risk factor for death <i>per se</i>. Rather, especially in the case of sepsis, clinically apparent positive fluid balance does not seem to be a disadvantage in terms of survival, KRT, and ROKF.</p>","PeriodicalId":94329,"journal":{"name":"Journal of clinical medicine research","volume":"16 6","pages":"302-309"},"PeriodicalIF":2.0000,"publicationDate":"2024-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11254307/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of clinical medicine research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr5190","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/30 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute kidney injury (AKI) is a common issue among in-hospital patients, with high mortality rates. Sepsis is a primary cause of AKI, particularly in the intensive care unit. Patients with septic AKI often experience cardiovascular congestion, leading to the formal classification of cardiorenal syndrome type 5. The study aimed to evaluate the prognosis of septic AKI patients with and without clinical evidence of cardiovascular congestion.
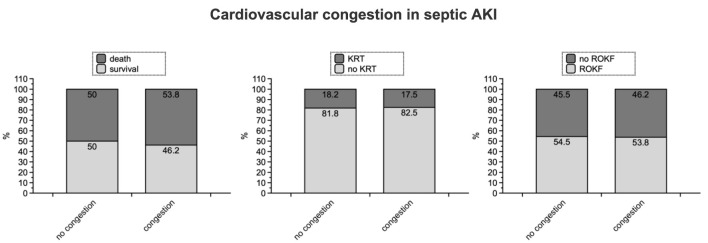
Methods: This was a retrospective observational study. AKI patients were identified using the in-hospital AKI alert system. Sepsis was diagnosed based on laboratory, clinical, and hemodynamic characteristics, with additional consideration of the quickSOFA score. Cardiovascular congestion was diagnosed by assessing clinical (edema), radiographic (pulmonary congestion), echocardiographic (e.g., wall motion abnormalities), and laboratory variables (e.g., N-terminal pro-B-type natriuretic peptide). Endpoints included in-hospital survival, the need for kidney replacement therapy (KRT), and recovery of kidney function (ROKF).
Results: In total, 102 patients were included, and cardiopulmonary congestion was diagnosed in 78.4%. Individuals with congestion did not differ from patients without congestion in any of the pre-defined endpoints.
Conclusions: It is justified not to consider clinically apparent cardiovascular congestion in septic AKI patients as a risk factor for death per se. Rather, especially in the case of sepsis, clinically apparent positive fluid balance does not seem to be a disadvantage in terms of survival, KRT, and ROKF.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
