{"title":"Can short- and long-term maternal and infant risks linked to hypertension and diabetes during pregnancy be reduced by therapy?","authors":"Olof Stephansson, Anna Sandström","doi":"10.1111/joim.13823","DOIUrl":null,"url":null,"abstract":"<p>Hypertensive disorders of pregnancy (HDP), especially preeclampsia, and diabetes during pregnancy pose significant risks for both maternal and infant health, extending to long-term outcomes such as early-onset cardiovascular disease and metabolic disorders. Current strategies for managing HDP focus on screening, prevention, surveillance, and timely intervention. No disease-modifying therapies exist so far for established preeclampsia; delivery remains the definitive resolution. Preventive measures—including early pregnancy screening, exercise, and low-dose aspirin—show promise. Antihypertensive treatments reduce severe hypertension risks, whereas magnesium sulfate remains the standard for preventing eclampsia. Planned delivery from gestational week 37 can balance maternal benefits and neonatal risks in women with established preeclampsia. Delivery between 34 and 37 weeks gestation in women with preeclampsia has to balance risks for mother and infant. Lifestyle interventions—particularly diet and physical activity—are pivotal in managing gestational diabetes mellitus and type 2 diabetes. The oral antidiabetic metformin has shown benefits in glycaemic control and reducing maternal weight gain, although its long-term effects on offspring remain uncertain. The safety of other peroral antidiabetics in pregnancy is less studied. Advancements in glucose monitoring and insulin administration present encouraging prospects for enhancing outcomes in women with diabetes types 1 and 2. Both HDP and diabetes during pregnancy necessitate vigilant management through a combination of lifestyle modifications, pharmacological interventions, and timely obstetric care. Although certain treatments such as low-dose aspirin and metformin show efficacy in risk reduction, further research is ongoing to ensure safety for both mothers and their offspring to reduce short- and long-term adverse effects.</p>","PeriodicalId":196,"journal":{"name":"Journal of Internal Medicine","volume":"296 3","pages":"216-233"},"PeriodicalIF":9.0000,"publicationDate":"2024-07-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/joim.13823","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Internal Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/joim.13823","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
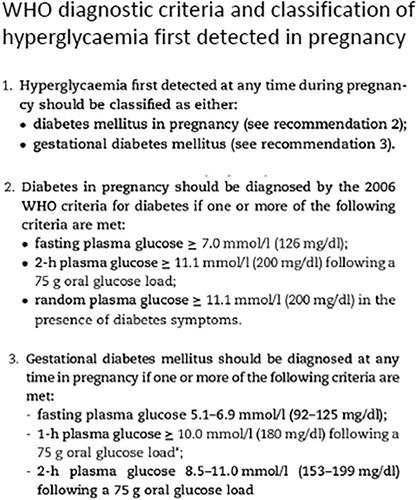
Hypertensive disorders of pregnancy (HDP), especially preeclampsia, and diabetes during pregnancy pose significant risks for both maternal and infant health, extending to long-term outcomes such as early-onset cardiovascular disease and metabolic disorders. Current strategies for managing HDP focus on screening, prevention, surveillance, and timely intervention. No disease-modifying therapies exist so far for established preeclampsia; delivery remains the definitive resolution. Preventive measures—including early pregnancy screening, exercise, and low-dose aspirin—show promise. Antihypertensive treatments reduce severe hypertension risks, whereas magnesium sulfate remains the standard for preventing eclampsia. Planned delivery from gestational week 37 can balance maternal benefits and neonatal risks in women with established preeclampsia. Delivery between 34 and 37 weeks gestation in women with preeclampsia has to balance risks for mother and infant. Lifestyle interventions—particularly diet and physical activity—are pivotal in managing gestational diabetes mellitus and type 2 diabetes. The oral antidiabetic metformin has shown benefits in glycaemic control and reducing maternal weight gain, although its long-term effects on offspring remain uncertain. The safety of other peroral antidiabetics in pregnancy is less studied. Advancements in glucose monitoring and insulin administration present encouraging prospects for enhancing outcomes in women with diabetes types 1 and 2. Both HDP and diabetes during pregnancy necessitate vigilant management through a combination of lifestyle modifications, pharmacological interventions, and timely obstetric care. Although certain treatments such as low-dose aspirin and metformin show efficacy in risk reduction, further research is ongoing to ensure safety for both mothers and their offspring to reduce short- and long-term adverse effects.
期刊介绍:
JIM – The Journal of Internal Medicine, in continuous publication since 1863, is an international, peer-reviewed scientific journal. It publishes original work in clinical science, spanning from bench to bedside, encompassing a wide range of internal medicine and its subspecialties. JIM showcases original articles, reviews, brief reports, and research letters in the field of internal medicine.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
