{"title":"Futility of Up-Front Resection for Anatomically Resectable Pancreatic Cancer.","authors":"Stefano Crippa, Giuseppe Malleo, Vincenzo Mazzaferro, Serena Langella, Claudio Ricci, Fabio Casciani, Giulio Belfiori, Sara Galati, Vincenzo D'Ambra, Gabriella Lionetto, Alessandro Ferrero, Riccardo Casadei, Giorgio Ercolani, Roberto Salvia, Massimo Falconi, Alessandro Cucchetti","doi":"10.1001/jamasurg.2024.2485","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>There are currently no clinically relevant criteria to predict a futile up-front pancreatectomy in patients with anatomically resectable pancreatic ductal adenocarcinoma.</p><p><strong>Objectives: </strong>To develop a futility risk model using a multi-institutional database and provide unified criteria associated with a futility likelihood below a safety threshold of 20%.</p><p><strong>Design, setting, and participants: </strong>This retrospective study took place from January 2010 through December 2021 at 5 high- or very high-volume centers in Italy. Data were analyzed during April 2024. Participants included consecutive patients undergoing up-front pancreatectomy at the participating institutions.</p><p><strong>Exposure: </strong>Standard management, per existing guidelines.</p><p><strong>Main outcomes and measures: </strong>The main outcome measure was the rate of futile pancreatectomy, defined as an operation resulting in patient death or disease recurrence within 6 months. Dichotomous criteria were constructed to maintain the futility likelihood below 20%, corresponding to the chance of not receiving postneoadjuvant resection from existing pooled data.</p><p><strong>Results: </strong>This study included 1426 patients. The median age was 69 (interquartile range, 62-75) years, 759 patients were male (53.2%), and 1076 had head cancer (75.4%). The rate of adjuvant treatment receipt was 73.7%. For the model construction, the study sample was split into a derivation (n = 885) and a validation cohort (n = 541). The rate of futile pancreatectomy was 18.9% (19.2% in the development and 18.6% in the validation cohort). Preoperative variables associated with futile resection were American Society of Anesthesiologists class (95% CI for coefficients, 0.68-0.87), cancer antigen (CA) 19.9 serum levels (95% CI, for coefficients 0.05-0.75), and tumor size (95% CI for coefficients, 0.28-0.46). Three risk groups associated with an escalating likelihood of futile resection, worse pathological features, and worse outcomes were identified. Four discrete conditions (defined as CA 19.9 levels-adjusted-to-size criteria: tumor size less than 2 cm with CA 19.9 levels less than 1000 U/mL; tumor size less than 3 cm with CA 19.9 levels less than 500 U/mL; tumor size less than 4 cm with CA 19.9 levels less than 150 U/mL; and tumor size less than 5 cm with CA 19.9 levels less than 50 U/mL) were associated with a futility likelihood below 20%. Both disease-free survival and overall survival were significantly longer in patients fulfilling the criteria.</p><p><strong>Conclusions and relevance: </strong>In this study, a preoperative model (MetroPancreas) and dichotomous criteria to determine the risk of futile pancreatectomy were developed. This might help in selecting patients for up-front resection or neoadjuvant therapy.</p>","PeriodicalId":14690,"journal":{"name":"JAMA surgery","volume":" ","pages":"1139-1147"},"PeriodicalIF":14.9000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11270270/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1001/jamasurg.2024.2485","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: There are currently no clinically relevant criteria to predict a futile up-front pancreatectomy in patients with anatomically resectable pancreatic ductal adenocarcinoma.
Objectives: To develop a futility risk model using a multi-institutional database and provide unified criteria associated with a futility likelihood below a safety threshold of 20%.
Design, setting, and participants: This retrospective study took place from January 2010 through December 2021 at 5 high- or very high-volume centers in Italy. Data were analyzed during April 2024. Participants included consecutive patients undergoing up-front pancreatectomy at the participating institutions.
Exposure: Standard management, per existing guidelines.
Main outcomes and measures: The main outcome measure was the rate of futile pancreatectomy, defined as an operation resulting in patient death or disease recurrence within 6 months. Dichotomous criteria were constructed to maintain the futility likelihood below 20%, corresponding to the chance of not receiving postneoadjuvant resection from existing pooled data.
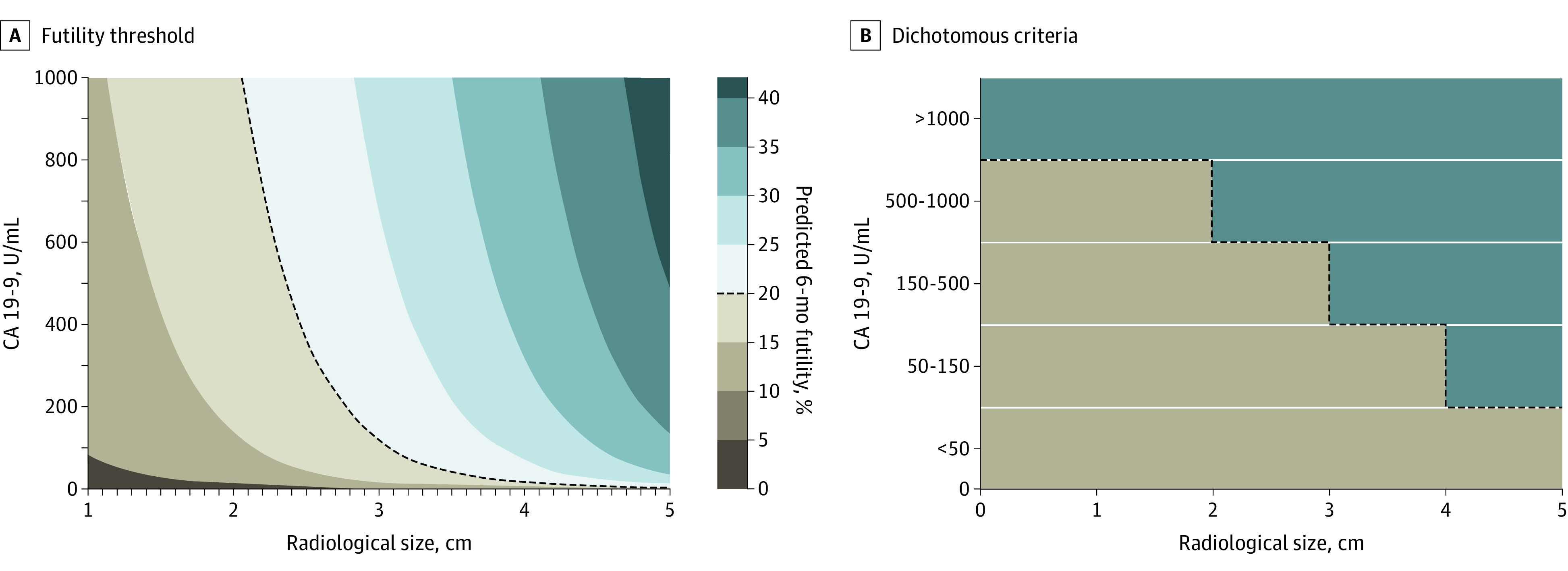
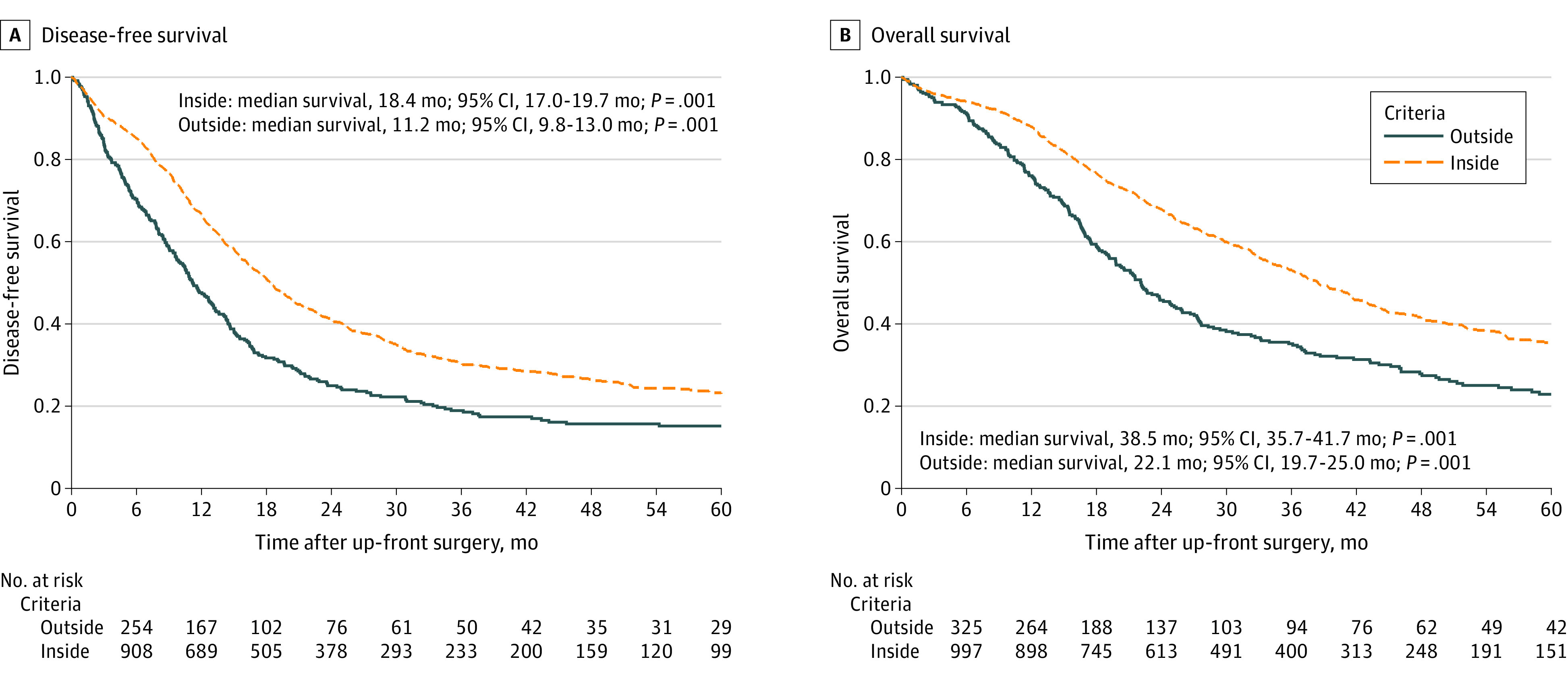
Results: This study included 1426 patients. The median age was 69 (interquartile range, 62-75) years, 759 patients were male (53.2%), and 1076 had head cancer (75.4%). The rate of adjuvant treatment receipt was 73.7%. For the model construction, the study sample was split into a derivation (n = 885) and a validation cohort (n = 541). The rate of futile pancreatectomy was 18.9% (19.2% in the development and 18.6% in the validation cohort). Preoperative variables associated with futile resection were American Society of Anesthesiologists class (95% CI for coefficients, 0.68-0.87), cancer antigen (CA) 19.9 serum levels (95% CI, for coefficients 0.05-0.75), and tumor size (95% CI for coefficients, 0.28-0.46). Three risk groups associated with an escalating likelihood of futile resection, worse pathological features, and worse outcomes were identified. Four discrete conditions (defined as CA 19.9 levels-adjusted-to-size criteria: tumor size less than 2 cm with CA 19.9 levels less than 1000 U/mL; tumor size less than 3 cm with CA 19.9 levels less than 500 U/mL; tumor size less than 4 cm with CA 19.9 levels less than 150 U/mL; and tumor size less than 5 cm with CA 19.9 levels less than 50 U/mL) were associated with a futility likelihood below 20%. Both disease-free survival and overall survival were significantly longer in patients fulfilling the criteria.
Conclusions and relevance: In this study, a preoperative model (MetroPancreas) and dichotomous criteria to determine the risk of futile pancreatectomy were developed. This might help in selecting patients for up-front resection or neoadjuvant therapy.
期刊介绍:
JAMA Surgery, an international peer-reviewed journal established in 1920, is the official publication of the Association of VA Surgeons, the Pacific Coast Surgical Association, and the Surgical Outcomes Club.It is a proud member of the JAMA Network, a consortium of peer-reviewed general medical and specialty publications.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
