Eisen Liang, Razeen Parvez, Sylvia Ng, Bevan Brown
{"title":"Uterine artery embolisation for adenomyosis in women who failed prior endometrial ablation","authors":"Eisen Liang, Razeen Parvez, Sylvia Ng, Bevan Brown","doi":"10.1186/s42155-024-00471-5","DOIUrl":null,"url":null,"abstract":"<p>To report the effectiveness of uterine artery embolisation (UAE) in treating adenomyosis in women who failed prior endometrial ablation (EA).</p><p>Endometrial ablation (EA) is a minimally invasive treatment for heavy menstrual bleeding (HMB). Patient satisfaction rates for EA are around 80–90%; however, about 10–20% of women require additional intervention (re-ablation or hysterectomy) due to persistent bleeding or pain [1]. Women with adenomyosis are more likely to fail EA [2]. Those with unsatisfactory outcomes from EA may be offered hysterectomy as their only remaining treatment option. Case series and meta-analyses have demonstrated that UAE is effective in alleviating adenomyosis-related HMB and dysmenorrhea [3, 4]. However, the effectiveness of UAE in treating women who failed prior EA has not been previously reported. This is a retrospective cohort study of the outcome of UAE for adenomyosis in women who failed previous EA.</p><p>This study was approved by the institutional Human Research Ethics Committee. Informed consent was obtained from each participant. Women presenting to our clinic with significant dysmenorrhea and/or HMB following unsatisfactory endometrial ablation were offered UAE as an alternative to hysterectomy. Medical records of women who had UAE for adenomyosis at our institution between January 2017 and March 2022 were reviewed to identify those who had EA prior to UAE. All women had pre-UAE MRI to confirm the presence of adenomyosis, diagnosed based on previously published criteria: junctional zone thickness of ≥ 12 mm or > 40% of myometrial thickness, or the presence of T2 hyperintense cysts/foci/fissuring [5]. All UAE procedures were performed with non-spherical polyvinyl alcohol (nsPVA) particles as previously described [4], and with starting nsPVA size at 180–300 micron (Cook 200) or 150–250 micron (Boston Scientific) as suggested by the 1-2-3 Protocol [6]. To evaluate the clinical outcome, a 2-part online survey was sent to women via email link to complete at home. Part 1 inquired about symptoms, menopausal status, overall satisfaction, and requirement for further intervention (Appendix 1). Women who had heavy menstrual bleeding prior to UAE were asked about their periods at the time of the audit. Overall success rate of UAE was assessed by asking women if they were “Very Satisfied,” “Satisfied,” “Not sure,” “Not Satisfied,” or “Very Unsatisfied” about the outcome. Only women who rated “Very Satisfied” or “Satisfied” were regarded as overall successful. Part 2 consisted of the validated Uterine Fibroid Symptom and Quality of Life Survey (UFSQoL) [7]. The following parameters before UAE and at follow-up were recorded and compared: dysmenorrhea visual analogue scale (VAS) pain score, number of days with dysmenorrhea, symptom score, and QoL score (using UFSQoL). Uterine volume and junctional zone thickness at baseline MRI and 6 months follow-up were compared. Significance of changes before and after treatment was analyzed using T-tests.</p><p>Between January 2017 and March 2022, UAE procedures were performed in 270 women for adenomyosis, some of whom also had fibroids. Eighteen women were identified with prior ablation failure (see Table 1): 15 with pure adenomyosis and 3 with coexisting fibroids. One woman was lost to follow-up; the outcomes of 17/18 (94.4%) were available for analysis, at a mean follow-up of 1.6 years post-UAE (median 2, range 0.6–3 years). Significant reductions in pain score (VAS 6.29), number of days in pain (2.6 days), symptom score (32.1/100), and significant improvement in QoL (39/100) were noted (Table 2). For the 8 women who still had HMB post-ablation, 7 (87.5%) saw significant improvement. Overall, 15/17 patients (88.2%) were “Satisfied” or “Very Satisfied” with the outcome of the UAE procedure (Fig. 1). Only 1 (5.9%) woman required a hysterectomy. No other women required further intervention such as laparoscopy for residual pain/endometriosis. No women reported menopause. No immediate or long-term complications were noted in this audit. Thirteen women (76.5%) attended follow-up imaging (Fig. 2). Significant uterine volume reduction and JZ thickness reduction were noted (Table 2).\n</p><figure><figcaption><b data-test=\"table-caption\">Table 1 Baseline parameters</b></figcaption><span>Full size table</span><svg aria-hidden=\"true\" focusable=\"false\" height=\"16\" role=\"img\" width=\"16\"><use xlink:href=\"#icon-eds-i-chevron-right-small\" xmlns:xlink=\"http://www.w3.org/1999/xlink\"></use></svg></figure><figure><figcaption><b data-test=\"table-caption\">Table 2 Results: changes against baseline</b></figcaption><span>Full size table</span><svg aria-hidden=\"true\" focusable=\"false\" height=\"16\" role=\"img\" width=\"16\"><use xlink:href=\"#icon-eds-i-chevron-right-small\" xmlns:xlink=\"http://www.w3.org/1999/xlink\"></use></svg></figure><figure><figcaption><b data-test=\"figure-caption-text\">Fig. 1</b></figcaption><picture><source srcset=\"//media.springernature.com/lw685/springer-static/image/art%3A10.1186%2Fs42155-024-00471-5/MediaObjects/42155_2024_471_Fig1_HTML.png?as=webp\" type=\"image/webp\"/><img alt=\"figure 1\" aria-describedby=\"Fig1\" height=\"787\" loading=\"lazy\" src=\"//media.springernature.com/lw685/springer-static/image/art%3A10.1186%2Fs42155-024-00471-5/MediaObjects/42155_2024_471_Fig1_HTML.png\" width=\"685\"/></picture><p><b>a</b> Results: Menstrual bleeding Post UAE. <b>b</b> Results: Overall outcome</p><span>Full size image</span><svg aria-hidden=\"true\" focusable=\"false\" height=\"16\" role=\"img\" width=\"16\"><use xlink:href=\"#icon-eds-i-chevron-right-small\" xmlns:xlink=\"http://www.w3.org/1999/xlink\"></use></svg></figure><figure><figcaption><b data-test=\"figure-caption-text\">Fig. 2</b></figcaption><picture><source srcset=\"//media.springernature.com/lw685/springer-static/image/art%3A10.1186%2Fs42155-024-00471-5/MediaObjects/42155_2024_471_Fig2_HTML.png?as=webp\" type=\"image/webp\"/><img alt=\"figure 2\" aria-describedby=\"Fig2\" height=\"888\" loading=\"lazy\" src=\"//media.springernature.com/lw685/springer-static/image/art%3A10.1186%2Fs42155-024-00471-5/MediaObjects/42155_2024_471_Fig2_HTML.png\" width=\"685\"/></picture><p>MRI of a 50-year-old woman who had endometrial ablation 10 months ago but was still suffering from heavy menstrual bleeding and severe dysmenorrhea. Following UAE, she had regular periods with lightest-ever bleeding and a reduction of pain score from 10 to 1. Sagittal T2 MRI pre- and post-embolisation demonstrated a reduction of uterine volume from 210 to 97 mL, reduction of junctional zone from 21 to 14 mm, less bulging globular appearance, and marked reduction of myometrial cystic spaces (ectopic endometrial tissue)</p><span>Full size image</span><svg aria-hidden=\"true\" focusable=\"false\" height=\"16\" role=\"img\" width=\"16\"><use xlink:href=\"#icon-eds-i-chevron-right-small\" xmlns:xlink=\"http://www.w3.org/1999/xlink\"></use></svg></figure><p>The woman who failed UAE requiring subsequent hysterectomy had pure diffuse adenomyosis and scored the smallest uterine volume (62 mL) of the study cohort. Her angiography showed low uterine vascularity and bilateral small uterine arteries, which were pretreated with 100 µg of glycerol trinitrate on each side, prior to embolisation with nsPVA (Cook 200).</p><p>This study has shown that UAE can be an effective treatment for post-ablation adenomyosis, with significant improvement in pain and residual HMB. Overall patient satisfaction is 88.2%, and 94.1% were able to avoid a hysterectomy. The results from this post-ablation failure cohort compare favourably with previously reported overall UAE outcomes for adenomyosis [3, 4]. UAE as a non-targeted particle embolisation causes global ischemia of uterus. We postulate that normal myometrium can recover and remains viable due to numerous underlying dormant collateral vessels that can be recruited; abnormal tissue like adenomyosis does not have spare vessels to recruit and will undergo irreversible ischaemic infarction.</p><p>The question of whether EA is appropriate to treat adenomyosis should be raised. Depth of involvement of adenomyosis has been shown to be associated with endometrial ablation failure [8]. Deep adenomyosis (> 2.5 mm) is present in a significant number of women who underwent hysterectomy after failed endometrial ablation [2]. EA devices are designed to cause thermal destruction of 4–6 mm depth of tissue to the basalis level [9]. MRI diagnosis of adenomyosis requires junctional zone thickness of 12 mm or more [5]. Therefore, if the diagnosis of adenomyosis is established based on MRI criteria, there is a high chance that endometrial ablation might fail. We strongly argue that if adenomyosis is established on imaging, UAE should be offered to women as an alternative to hysterectomy, as many case series has demonstrated the safety and effectiveness of UAE for adenomyosis [3, 4]. Previous studies suggest that ablation either activates surviving endometrial tissue to penetrate the myometrium, causing adenomyosis, or activates embedded ectopic endometrial glands to grow deeper into the myometrium, resulting in deeper adenomyosis [8]. This might explain dysmenorrhea as a main clinical feature of EA failure that requires further intervention. Women with dysmenorrhea might have endometriosis and/or adenomyosis and are therefore at risk of persistent pelvic pain after endometrial ablation, which treats neither of the two underlying conditions. The presence of pre-existing dysmenorrhea is the most strongly correlated risk factor for receiving a surgical reintervention such as hysterectomy [1]. Women’s health practitioners should be aware that failure to correctly diagnose adenomyosis might result in the inadvertent use of ablation, leading to further intervention. Improved diagnostic accuracy of adenomyosis may reduce the number of women undergoing inappropriate ablation. This might require wider use of MRI, which has a higher sensitivity and specificity than ultrasound in diagnosing adenomyosis [10]. This is a small retrospective cohort study. The average follow-up of 1.6 years remains short, and the longer-term hysterectomy rate is yet to be defined by future studies. It is not known if the adenomyosis was present prior to EA or developed subsequent to EA. There is no pathological proof of the underlying pathology being treated by UAE. Future studies could be designed to use MRI to document the absence of adenomyosis prior to EA and see if there is a reduction in EA failure rate.</p><p>UAE is safe and effective in managing women who failed endometrial ablation, with significant improvement in dysmenorrhea and heavy menstrual bleeding. Most women were able to avoid hysterectomy following UAE for ablation failure.</p><p>Data is available for review upon request.</p><ol data-track-component=\"outbound reference\" data-track-context=\"references section\"><li data-counter=\"1.\"><p>Beelen PP, Reinders WIM, Scheepers CFWM, Herman JM, Geomini PMA, Van Kuijk YMCM, Bongers MY. Prognostic factors for the failure of endometrial ablation: a systematic review and meta-analysis. Obstet Gynecol. 2019;134(6):1269–81.</p><p>Article PubMed Google Scholar </p></li><li data-counter=\"2.\"><p>Mengerink BB, van der Wurff AAM, ter Haar JF, van Rooij IA, Pijnenborg JMA. Effect of undiagnosed deep adenomyosis after failed novasure endometrial ablation. J Minim Invasive Gynecol. 2015;22:239–44.</p><p>Article PubMed Google Scholar </p></li><li data-counter=\"3.\"><p>de Bruijn AM, Smink M, Lohle PNM, Huirne JAF, Twisk JWR, Wong C, Schoonmade L, Hehenkamp WJK. Uterine artery embolization for the treatment of adenomyosis: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017;28:1629–42.</p><p>Article PubMed Google Scholar </p></li><li data-counter=\"4.\"><p>Liang E, Brown B, Rachinski M. A clinical audit on the efficacy and safety of uterine artery embolisation for symptomatic adenomyosis: results in 117 women. Aust N Z J Obstet Gynaecol. 2018;58:454–9.</p><p>Article PubMed Google Scholar </p></li><li data-counter=\"5.\"><p>Agostinho L, Cruz R, Osório F, Alves J, Setúbal A, Guerra A. MRI for adenomyosis: a pictorial review. Insights Imaging. 2017. https://doi.org/10.1007/s13244-017-0576-z.</p><p>Article PubMed PubMed Central Google Scholar </p></li><li data-counter=\"6.\"><p>Kim MD, Kim YM, Kim HC, Cho JH, Kang HG, Lee C, Kim HJ, Lee JT. Uterine artery embolization for symptomatic adenomyosis: a new technical development of the 1-2-3 protocol and predictive factors of MR imaging affecting outcomes. J Vasc Interv Radiol. 2011;22(4):497–502.</p><p>Article PubMed Google Scholar </p></li><li data-counter=\"7.\"><p>Spies JB, Coyne K, Guaou Guaou N, et al. The UFS-QOL, a new disease-specific symptom and health-related quality of life questionnaire for leiomyomata. Obstet Gynecol. 2002;99(2):290–300.</p><p>PubMed Google Scholar </p></li><li data-counter=\"8.\"><p>McCausland AM, McCausland VM. Depth of endometrial penetration in adenomyosis helps determine outcome of rollerball ablation. Am J Obstet Gynecol. 1996;174:1786–94.</p><p>Article CAS PubMed Google Scholar </p></li><li data-counter=\"9.\"><p>Daub CA, Sepmeyer JA, Hathuc V, Sakala MD, Caserta MP, Clingan MJ, Hosseinzadeh K. Endometrial ablation: normal imaging appearance and delayed complications. Am J Roentgenol. 2015;205(4):W451–60.</p><p>Article Google Scholar </p></li><li data-counter=\"10.\"><p>Champaneria R, Abedin P, Daniels J, Balogun M, Khan KS. Ultrasound scan and magnetic resonance imaging for the diagnosis of adenomyosis: systematic review comparing test accuracy. Acta Obstet Gynecol Scand. 2010;89(11):1374–84.</p><p>Article PubMed Google Scholar </p></li></ol><p>Download references<svg aria-hidden=\"true\" focusable=\"false\" height=\"16\" role=\"img\" width=\"16\"><use xlink:href=\"#icon-eds-i-download-medium\" xmlns:xlink=\"http://www.w3.org/1999/xlink\"></use></svg></p><p>No special acknowledgements.</p><p>There was no financial support from outside organisation.</p><h3>Authors and Affiliations</h3><ol><li><p>Sydney Fibroid Clinic, Sydney, Australia</p><p>Eisen Liang, Razeen Parvez & Bevan Brown</p></li><li><p>Gosford Hospital, Gosford, NSW, Australia</p><p>Sylvia Ng</p></li></ol><span>Authors</span><ol><li><span>Eisen Liang</span>View author publications<p>You can also search for this author in <span>PubMed<span> </span>Google Scholar</span></p></li><li><span>Razeen Parvez</span>View author publications<p>You can also search for this author in <span>PubMed<span> </span>Google Scholar</span></p></li><li><span>Sylvia Ng</span>View author publications<p>You can also search for this author in <span>PubMed<span> </span>Google Scholar</span></p></li><li><span>Bevan Brown</span>View author publications<p>You can also search for this author in <span>PubMed<span> </span>Google Scholar</span></p></li></ol><h3>Contributions</h3><p>Authors’ contribution are as follows: Eisen Liang’s role: design concept, ethics submission data collection, literature review, drafting of paper, submission. Razeen Parvez’s role: data collection, data analysis, literature search, ethics submission. Sylvia Ng’s role: data analysis, literature search, drafting / formatting/ referencing, Bevan Brown’s role: design concept, literature review, review of draft and editing.</p>\n<h3>Authors’ information</h3>\n<p>Eisen Liang: Interventional Radiologist.</p>\n<p>Razeen Parvez: Research Assistant, Medical student.</p>\n<p>Sylvia Ng: Research Assistant, Radiology Trainee.</p>\n<p>Bevan Brown: Gynaecologist.</p>\n<h3>Corresponding author</h3><p>Correspondence to Eisen Liang.</p><h3>Ethics approval and consent to participate</h3>\n<p>Informed consent was obtained from all individual participants involved in the study.</p>\n<p>This study was approved by the Adventist HealthCare Limited Human Research Ethics Committee (HREC 2022–028).</p>\n<h3>Consent for publication</h3>\n<p>We consent for publication in CVIR Endovascular.</p>\n<h3>Competing interests</h3>\n<p>There is no conflict of interest identified.</p><h3>Publisher’s Note</h3><p>Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.</p><h3>Supplementary Material 1.</h3><p><b>Open Access</b> This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.</p>\n<p>Reprints and permissions</p><img alt=\"Check for updates. Verify currency and authenticity via CrossMark\" height=\"81\" loading=\"lazy\" src=\"data:image/svg+xml;base64,PHN2ZyBoZWlnaHQ9IjgxIiB3aWR0aD0iNTciIHhtbG5zPSJodHRwOi8vd3d3LnczLm9yZy8yMDAwL3N2ZyI+PGcgZmlsbD0ibm9uZSIgZmlsbC1ydWxlPSJldmVub2RkIj48cGF0aCBkPSJtMTcuMzUgMzUuNDUgMjEuMy0xNC4ydi0xNy4wM2gtMjEuMyIgZmlsbD0iIzk4OTg5OCIvPjxwYXRoIGQ9Im0zOC42NSAzNS40NS0yMS4zLTE0LjJ2LTE3LjAzaDIxLjMiIGZpbGw9IiM3NDc0NzQiLz48cGF0aCBkPSJtMjggLjVjLTEyLjk4IDAtMjMuNSAxMC41Mi0yMy41IDIzLjVzMTAuNTIgMjMuNSAyMy41IDIzLjUgMjMuNS0xMC41MiAyMy41LTIzLjVjMC02LjIzLTIuNDgtMTIuMjEtNi44OC0xNi42Mi00LjQxLTQuNC0xMC4zOS02Ljg4LTE2LjYyLTYuODh6bTAgNDEuMjVjLTkuOCAwLTE3Ljc1LTcuOTUtMTcuNzUtMTcuNzVzNy45NS0xNy43NSAxNy43NS0xNy43NSAxNy43NSA3Ljk1IDE3Ljc1IDE3Ljc1YzAgNC43MS0xLjg3IDkuMjItNS4yIDEyLjU1cy03Ljg0IDUuMi0xMi41NSA1LjJ6IiBmaWxsPSIjNTM1MzUzIi8+PHBhdGggZD0ibTQxIDM2Yy01LjgxIDYuMjMtMTUuMjMgNy40NS0yMi40MyAyLjktNy4yMS00LjU1LTEwLjE2LTEzLjU3LTcuMDMtMjEuNWwtNC45Mi0zLjExYy00Ljk1IDEwLjctMS4xOSAyMy40MiA4Ljc4IDI5LjcxIDkuOTcgNi4zIDIzLjA3IDQuMjIgMzAuNi00Ljg2eiIgZmlsbD0iIzljOWM5YyIvPjxwYXRoIGQ9Im0uMiA1OC40NWMwLS43NS4xMS0xLjQyLjMzLTIuMDFzLjUyLTEuMDkuOTEtMS41Yy4zOC0uNDEuODMtLjczIDEuMzQtLjk0LjUxLS4yMiAxLjA2LS4zMiAxLjY1LS4zMi41NiAwIDEuMDYuMTEgMS41MS4zNS40NC4yMy44MS41IDEuMS44MWwtLjkxIDEuMDFjLS4yNC0uMjQtLjQ5LS40Mi0uNzUtLjU2LS4yNy0uMTMtLjU4LS4yLS45My0uMi0uMzkgMC0uNzMuMDgtMS4wNS4yMy0uMzEuMTYtLjU4LjM3LS44MS42Ni0uMjMuMjgtLjQxLjYzLS41MyAxLjA0LS4xMy40MS0uMTkuODgtLjE5IDEuMzkgMCAxLjA0LjIzIDEuODYuNjggMi40Ni40NS41OSAxLjA2Ljg4IDEuODQuODguNDEgMCAuNzctLjA3IDEuMDctLjIzcy41OS0uMzkuODUtLjY4bC45MSAxYy0uMzguNDMtLjguNzYtMS4yOC45OS0uNDcuMjItMSAuMzQtMS41OC4zNC0uNTkgMC0xLjEzLS4xLTEuNjQtLjMxLS41LS4yLS45NC0uNTEtMS4zMS0uOTEtLjM4LS40LS42Ny0uOS0uODgtMS40OC0uMjItLjU5LS4zMy0xLjI2LS4zMy0yLjAyem04LjQtNS4zM2gxLjYxdjIuNTRsLS4wNSAxLjMzYy4yOS0uMjcuNjEtLjUxLjk2LS43MnMuNzYtLjMxIDEuMjQtLjMxYy43MyAwIDEuMjcuMjMgMS42MS43MS4zMy40Ny41IDEuMTQuNSAyLjAydjQuMzFoLTEuNjF2LTQuMWMwLS41Ny0uMDgtLjk3LS4yNS0xLjIxLS4xNy0uMjMtLjQ1LS4zNS0uODMtLjM1LS4zIDAtLjU2LjA4LS43OS4yMi0uMjMuMTUtLjQ5LjM2LS43OC42NHY0LjhoLTEuNjF6bTcuMzcgNi40NWMwLS41Ni4wOS0xLjA2LjI2LTEuNTEuMTgtLjQ1LjQyLS44My43MS0xLjE0LjI5LS4zLjYzLS41NCAxLjAxLS43MS4zOS0uMTcuNzgtLjI1IDEuMTgtLjI1LjQ3IDAgLjg4LjA4IDEuMjMuMjQuMzYuMTYuNjUuMzguODkuNjdzLjQyLjYzLjU0IDEuMDNjLjEyLjQxLjE4Ljg0LjE4IDEuMzIgMCAuMzItLjAyLjU3LS4wNy43NmgtNC4zNmMuMDcuNjIuMjkgMS4xLjY1IDEuNDQuMzYuMzMuODIuNSAxLjM4LjUuMjkgMCAuNTctLjA0LjgzLS4xM3MuNTEtLjIxLjc2LS4zN2wuNTUgMS4wMWMtLjMzLjIxLS42OS4zOS0xLjA5LjUzLS40MS4xNC0uODMuMjEtMS4yNi4yMS0uNDggMC0uOTItLjA4LTEuMzQtLjI1LS40MS0uMTYtLjc2LS40LTEuMDctLjctLjMxLS4zMS0uNTUtLjY5LS43Mi0xLjEzLS4xOC0uNDQtLjI2LS45NS0uMjYtMS41MnptNC42LS42MmMwLS41NS0uMTEtLjk4LS4zNC0xLjI4LS4yMy0uMzEtLjU4LS40Ny0xLjA2LS40Ny0uNDEgMC0uNzcuMTUtMS4wNy40NS0uMzEuMjktLjUuNzMtLjU4IDEuM3ptMi41LjYyYzAtLjU3LjA5LTEuMDguMjgtMS41My4xOC0uNDQuNDMtLjgyLjc1LTEuMTNzLjY5LS41NCAxLjEtLjcxYy40Mi0uMTYuODUtLjI0IDEuMzEtLjI0LjQ1IDAgLjg0LjA4IDEuMTcuMjNzLjYxLjM0Ljg1LjU3bC0uNzcgMS4wMmMtLjE5LS4xNi0uMzgtLjI4LS41Ni0uMzctLjE5LS4wOS0uMzktLjE0LS42MS0uMTQtLjU2IDAtMS4wMS4yMS0xLjM1LjYzLS4zNS40MS0uNTIuOTctLjUyIDEuNjcgMCAuNjkuMTcgMS4yNC41MSAxLjY2LjM0LjQxLjc4LjYyIDEuMzIuNjIuMjggMCAuNTQtLjA2Ljc4LS4xNy4yNC0uMTIuNDUtLjI2LjY0LS40MmwuNjcgMS4wM2MtLjMzLjI5LS42OS41MS0xLjA4LjY1LS4zOS4xNS0uNzguMjMtMS4xOC4yMy0uNDYgMC0uOS0uMDgtMS4zMS0uMjQtLjQtLjE2LS43NS0uMzktMS4wNS0uN3MtLjUzLS42OS0uNy0xLjEzYy0uMTctLjQ1LS4yNS0uOTYtLjI1LTEuNTN6bTYuOTEtNi40NWgxLjU4djYuMTdoLjA1bDIuNTQtMy4xNmgxLjc3bC0yLjM1IDIuOCAyLjU5IDQuMDdoLTEuNzVsLTEuNzctMi45OC0xLjA4IDEuMjN2MS43NWgtMS41OHptMTMuNjkgMS4yN2MtLjI1LS4xMS0uNS0uMTctLjc1LS4xNy0uNTggMC0uODcuMzktLjg3IDEuMTZ2Ljc1aDEuMzR2MS4yN2gtMS4zNHY1LjZoLTEuNjF2LTUuNmgtLjkydi0xLjJsLjkyLS4wN3YtLjcyYzAtLjM1LjA0LS42OC4xMy0uOTguMDgtLjMxLjIxLS41Ny40LS43OXMuNDItLjM5LjcxLS41MWMuMjgtLjEyLjYzLS4xOCAxLjA0LS4xOC4yNCAwIC40OC4wMi42OS4wNy4yMi4wNS40MS4xLjU3LjE3em0uNDggNS4xOGMwLS41Ny4wOS0xLjA4LjI3LTEuNTMuMTctLjQ0LjQxLS44Mi43Mi0xLjEzLjMtLjMxLjY1LS41NCAxLjA0LS43MS4zOS0uMTYuOC0uMjQgMS4yMy0uMjRzLjg0LjA4IDEuMjQuMjRjLjQuMTcuNzQuNCAxLjA0Ljcxcy41NC42OS43MiAxLjEzYy4xOS40NS4yOC45Ni4yOCAxLjUzcy0uMDkgMS4wOC0uMjggMS41M2MtLjE4LjQ0LS40Mi44Mi0uNzIgMS4xM3MtLjY0LjU0LTEuMDQuNy0uODEuMjQtMS4yNC4yNC0uODQtLjA4LTEuMjMtLjI0LS43NC0uMzktMS4wNC0uN2MtLjMxLS4zMS0uNTUtLjY5LS43Mi0xLjEzLS4xOC0uNDUtLjI3LS45Ni0uMjctMS41M3ptMS42NSAwYzAgLjY5LjE0IDEuMjQuNDMgMS42Ni4yOC40MS42OC42MiAxLjE4LjYyLjUxIDAgLjktLjIxIDEuMTktLjYyLjI5LS40Mi40NC0uOTcuNDQtMS42NiAwLS43LS4xNS0xLjI2LS40NC0xLjY3LS4yOS0uNDItLjY4LS42My0xLjE5LS42My0uNSAwLS45LjIxLTEuMTguNjMtLjI5LjQxLS40My45Ny0uNDMgMS42N3ptNi40OC0zLjQ0aDEuMzNsLjEyIDEuMjFoLjA1Yy4yNC0uNDQuNTQtLjc5Ljg4LTEuMDIuMzUtLjI0LjctLjM2IDEuMDctLjM2LjMyIDAgLjU5LjA1Ljc4LjE0bC0uMjggMS40LS4zMy0uMDljLS4xMS0uMDEtLjIzLS4wMi0uMzgtLjAyLS4yNyAwLS41Ni4xLS44Ni4zMXMtLjU1LjU4LS43NyAxLjF2NC4yaC0xLjYxem0tNDcuODcgMTVoMS42MXY0LjFjMCAuNTcuMDguOTcuMjUgMS4yLjE3LjI0LjQ0LjM1LjgxLjM1LjMgMCAuNTctLjA3LjgtLjIyLjIyLS4xNS40Ny0uMzkuNzMtLjczdi00LjdoMS42MXY2Ljg3aC0xLjMybC0uMTItMS4wMWgtLjA0Yy0uMy4zNi0uNjMuNjQtLjk4Ljg2LS4zNS4yMS0uNzYuMzItMS4yNC4zMi0uNzMgMC0xLjI3LS4yNC0xLjYxLS43MS0uMzMtLjQ3LS41LTEuMTQtLjUtMi4wMnptOS40NiA3LjQzdjIuMTZoLTEuNjF2LTkuNTloMS4zM2wuMTIuNzJoLjA1Yy4yOS0uMjQuNjEtLjQ1Ljk3LS42My4zNS0uMTcuNzItLjI2IDEuMS0uMjYuNDMgMCAuODEuMDggMS4xNS4yNC4zMy4xNy42MS40Ljg0LjcxLjI0LjMxLjQxLjY4LjUzIDEuMTEuMTMuNDIuMTkuOTEuMTkgMS40NCAwIC41OS0uMDkgMS4xMS0uMjUgMS41Ny0uMTYuNDctLjM4Ljg1LS42NSAxLjE2LS4yNy4zMi0uNTguNTYtLjk0LjczLS4zNS4xNi0uNzIuMjUtMS4xLjI1LS4zIDAtLjYtLjA3LS45LS4ycy0uNTktLjMxLS44Ny0uNTZ6bTAtMi4zYy4yNi4yMi41LjM3LjczLjQ1LjI0LjA5LjQ2LjEzLjY2LjEzLjQ2IDAgLjg0LS4yIDEuMTUtLjYuMzEtLjM5LjQ2LS45OC40Ni0xLjc3IDAtLjY5LS4xMi0xLjIyLS4zNS0xLjYxLS4yMy0uMzgtLjYxLS41Ny0xLjEzLS41Ny0uNDkgMC0uOTkuMjYtMS41Mi43N3ptNS44Ny0xLjY5YzAtLjU2LjA4LTEuMDYuMjUtMS41MS4xNi0uNDUuMzctLjgzLjY1LTEuMTQuMjctLjMuNTgtLjU0LjkzLS43MXMuNzEtLjI1IDEuMDgtLjI1Yy4zOSAwIC43My4wNyAxIC4yLjI3LjE0LjU0LjMyLjgxLjU1bC0uMDYtMS4xdi0yLjQ5aDEuNjF2OS44OGgtMS4zM2wtLjExLS43NGgtLjA2Yy0uMjUuMjUtLjU0LjQ2LS44OC42NC0uMzMuMTgtLjY5LjI3LTEuMDYuMjctLjg3IDAtMS41Ni0uMzItMi4wNy0uOTVzLS43Ni0xLjUxLS43Ni0yLjY1em0xLjY3LS4wMWMwIC43NC4xMyAxLjMxLjQgMS43LjI2LjM4LjY1LjU4IDEuMTUuNTguNTEgMCAuOTktLjI2IDEuNDQtLjc3di0zLjIxYy0uMjQtLjIxLS40OC0uMzYtLjctLjQ1LS4yMy0uMDgtLjQ2LS4xMi0uNy0uMTItLjQ1IDAtLjgyLjE5LTEuMTMuNTktLjMxLjM5LS40Ni45NS0uNDYgMS42OHptNi4zNSAxLjU5YzAtLjczLjMyLTEuMy45Ny0xLjcxLjY0LS40IDEuNjctLjY4IDMuMDgtLjg0IDAtLjE3LS4wMi0uMzQtLjA3LS41MS0uMDUtLjE2LS4xMi0uMy0uMjItLjQzcy0uMjItLjIyLS4zOC0uM2MtLjE1LS4wNi0uMzQtLjEtLjU4LS4xLS4zNCAwLS42OC4wNy0xIC4ycy0uNjMuMjktLjkzLjQ3bC0uNTktMS4wOGMuMzktLjI0LjgxLS40NSAxLjI4LS42My40Ny0uMTcuOTktLjI2IDEuNTQtLjI2Ljg2IDAgMS41MS4yNSAxLjkzLjc2cy42MyAxLjI1LjYzIDIuMjF2NC4wN2gtMS4zMmwtLjEyLS43NmgtLjA1Yy0uMy4yNy0uNjMuNDgtLjk4LjY2cy0uNzMuMjctMS4xNC4yN2MtLjYxIDAtMS4xLS4xOS0xLjQ4LS41Ni0uMzgtLjM2LS41Ny0uODUtLjU3LTEuNDZ6bTEuNTctLjEyYzAgLjMuMDkuNTMuMjcuNjcuMTkuMTQuNDIuMjEuNzEuMjEuMjggMCAuNTQtLjA3Ljc3LS4ycy40OC0uMzEuNzMtLjU2di0xLjU0Yy0uNDcuMDYtLjg2LjEzLTEuMTguMjMtLjMxLjA5LS41Ny4xOS0uNzYuMzFzLS4zMy4yNS0uNDEuNGMtLjA5LjE1LS4xMy4zMS0uMTMuNDh6bTYuMjktMy42M2gtLjk4di0xLjJsMS4wNi0uMDcuMi0xLjg4aDEuMzR2MS44OGgxLjc1djEuMjdoLTEuNzV2My4yOGMwIC44LjMyIDEuMi45NyAxLjIuMTIgMCAuMjQtLjAxLjM3LS4wNC4xMi0uMDMuMjQtLjA3LjM0LS4xMWwuMjggMS4xOWMtLjE5LjA2LS40LjEyLS42NC4xNy0uMjMuMDUtLjQ5LjA4LS43Ni4wOC0uNCAwLS43NC0uMDYtMS4wMi0uMTgtLjI3LS4xMy0uNDktLjMtLjY3LS41Mi0uMTctLjIxLS4zLS40OC0uMzctLjc4LS4wOC0uMy0uMTItLjY0LS4xMi0xLjAxem00LjM2IDIuMTdjMC0uNTYuMDktMS4wNi4yNy0xLjUxcy40MS0uODMuNzEtMS4xNGMuMjktLjMuNjMtLjU0IDEuMDEtLjcxLjM5LS4xNy43OC0uMjUgMS4xOC0uMjUuNDcgMCAuODguMDggMS4yMy4yNC4zNi4xNi42NS4zOC44OS42N3MuNDIuNjMuNTQgMS4wM2MuMTIuNDEuMTguODQuMTggMS4zMiAwIC4zMi0uMDIuNTctLjA3Ljc2aC00LjM3Yy4wOC42Mi4yOSAxLjEuNjUgMS40NC4zNi4zMy44Mi41IDEuMzguNS4zIDAgLjU4LS4wNC44NC0uMTMuMjUtLjA5LjUxLS4yMS43Ni0uMzdsLjU0IDEuMDFjLS4zMi4yMS0uNjkuMzktMS4wOS41M3MtLjgyLjIxLTEuMjYuMjFjLS40NyAwLS45Mi0uMDgtMS4zMy0uMjUtLjQxLS4xNi0uNzctLjQtMS4wOC0uNy0uMy0uMzEtLjU0LS42OS0uNzItMS4xMy0uMTctLjQ0LS4yNi0uOTUtLjI2LTEuNTJ6bTQuNjEtLjYyYzAtLjU1LS4xMS0uOTgtLjM0LTEuMjgtLjIzLS4zMS0uNTgtLjQ3LTEuMDYtLjQ3LS40MSAwLS43Ny4xNS0xLjA4LjQ1LS4zMS4yOS0uNS43My0uNTcgMS4zem0zLjAxIDIuMjNjLjMxLjI0LjYxLjQzLjkyLjU3LjMuMTMuNjMuMi45OC4yLjM4IDAgLjY1LS4wOC44My0uMjNzLjI3LS4zNS4yNy0uNmMwLS4xNC0uMDUtLjI2LS4xMy0uMzctLjA4LS4xLS4yLS4yLS4zNC0uMjgtLjE0LS4wOS0uMjktLjE2LS40Ny0uMjNsLS41My0uMjJjLS4yMy0uMDktLjQ2LS4xOC0uNjktLjMtLjIzLS4xMS0uNDQtLjI0LS42Mi0uNHMtLjMzLS4zNS0uNDUtLjU1Yy0uMTItLjIxLS4xOC0uNDYtLjE4LS43NSAwLS42MS4yMy0xLjEuNjgtMS40OS40NC0uMzggMS4wNi0uNTcgMS44My0uNTcuNDggMCAuOTEuMDggMS4yOS4yNXMuNzEuMzYuOTkuNTdsLS43NC45OGMtLjI0LS4xNy0uNDktLjMyLS43My0uNDItLjI1LS4xMS0uNTEtLjE2LS43OC0uMTYtLjM1IDAtLjYuMDctLjc2LjIxLS4xNy4xNS0uMjUuMzMtLjI1LjU0IDAgLjE0LjA0LjI2LjEyLjM2cy4xOC4xOC4zMS4yNmMuMTQuMDcuMjkuMTQuNDYuMjFsLjU0LjE5Yy4yMy4wOS40Ny4xOC43LjI5cy40NC4yNC42NC40Yy4xOS4xNi4zNC4zNS40Ni41OC4xMS4yMy4xNy41LjE3LjgyIDAgLjMtLjA2LjU4LS4xNy44My0uMTIuMjYtLjI5LjQ4LS41MS42OC0uMjMuMTktLjUxLjM0LS44NC40NS0uMzQuMTEtLjcyLjE3LTEuMTUuMTctLjQ4IDAtLjk1LS4wOS0xLjQxLS4yNy0uNDYtLjE5LS44Ni0uNDEtMS4yLS42OHoiIGZpbGw9IiM1MzUzNTMiLz48L2c+PC9zdmc+\" width=\"57\"/><h3>Cite this article</h3><p>Liang, E., Parvez, R., Ng, S. <i>et al.</i> Uterine artery embolisation for adenomyosis in women who failed prior endometrial ablation. <i>CVIR Endovasc</i> <b>7</b>, 59 (2024). https://doi.org/10.1186/s42155-024-00471-5</p><p>Download citation<svg aria-hidden=\"true\" focusable=\"false\" height=\"16\" role=\"img\" width=\"16\"><use xlink:href=\"#icon-eds-i-download-medium\" xmlns:xlink=\"http://www.w3.org/1999/xlink\"></use></svg></p><ul data-test=\"publication-history\"><li><p>Received<span>: </span><span><time datetime=\"2024-06-08\">08 June 2024</time></span></p></li><li><p>Accepted<span>: </span><span><time datetime=\"2024-07-10\">10 July 2024</time></span></p></li><li><p>Published<span>: </span><span><time datetime=\"2024-07-27\">27 July 2024</time></span></p></li><li><p>DOI</abbr><span>: </span><span>https://doi.org/10.1186/s42155-024-00471-5</span></p></li></ul><h3>Share this article</h3><p>Anyone you share the following link with will be able to read this content:</p><button data-track=\"click\" data-track-action=\"get shareable link\" data-track-external=\"\" data-track-label=\"button\" type=\"button\">Get shareable link</button><p>Sorry, a shareable link is not currently available for this article.</p><p data-track=\"click\" data-track-action=\"select share url\" data-track-label=\"button\"></p><button data-track=\"click\" data-track-action=\"copy share url\" data-track-external=\"\" data-track-label=\"button\" type=\"button\">Copy to clipboard</button><p> Provided by the Springer Nature SharedIt content-sharing initiative </p>","PeriodicalId":52351,"journal":{"name":"CVIR Endovascular","volume":"37 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-07-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"CVIR Endovascular","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s42155-024-00471-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
To report the effectiveness of uterine artery embolisation (UAE) in treating adenomyosis in women who failed prior endometrial ablation (EA).
Endometrial ablation (EA) is a minimally invasive treatment for heavy menstrual bleeding (HMB). Patient satisfaction rates for EA are around 80–90%; however, about 10–20% of women require additional intervention (re-ablation or hysterectomy) due to persistent bleeding or pain [1]. Women with adenomyosis are more likely to fail EA [2]. Those with unsatisfactory outcomes from EA may be offered hysterectomy as their only remaining treatment option. Case series and meta-analyses have demonstrated that UAE is effective in alleviating adenomyosis-related HMB and dysmenorrhea [3, 4]. However, the effectiveness of UAE in treating women who failed prior EA has not been previously reported. This is a retrospective cohort study of the outcome of UAE for adenomyosis in women who failed previous EA.
This study was approved by the institutional Human Research Ethics Committee. Informed consent was obtained from each participant. Women presenting to our clinic with significant dysmenorrhea and/or HMB following unsatisfactory endometrial ablation were offered UAE as an alternative to hysterectomy. Medical records of women who had UAE for adenomyosis at our institution between January 2017 and March 2022 were reviewed to identify those who had EA prior to UAE. All women had pre-UAE MRI to confirm the presence of adenomyosis, diagnosed based on previously published criteria: junctional zone thickness of ≥ 12 mm or > 40% of myometrial thickness, or the presence of T2 hyperintense cysts/foci/fissuring [5]. All UAE procedures were performed with non-spherical polyvinyl alcohol (nsPVA) particles as previously described [4], and with starting nsPVA size at 180–300 micron (Cook 200) or 150–250 micron (Boston Scientific) as suggested by the 1-2-3 Protocol [6]. To evaluate the clinical outcome, a 2-part online survey was sent to women via email link to complete at home. Part 1 inquired about symptoms, menopausal status, overall satisfaction, and requirement for further intervention (Appendix 1). Women who had heavy menstrual bleeding prior to UAE were asked about their periods at the time of the audit. Overall success rate of UAE was assessed by asking women if they were “Very Satisfied,” “Satisfied,” “Not sure,” “Not Satisfied,” or “Very Unsatisfied” about the outcome. Only women who rated “Very Satisfied” or “Satisfied” were regarded as overall successful. Part 2 consisted of the validated Uterine Fibroid Symptom and Quality of Life Survey (UFSQoL) [7]. The following parameters before UAE and at follow-up were recorded and compared: dysmenorrhea visual analogue scale (VAS) pain score, number of days with dysmenorrhea, symptom score, and QoL score (using UFSQoL). Uterine volume and junctional zone thickness at baseline MRI and 6 months follow-up were compared. Significance of changes before and after treatment was analyzed using T-tests.
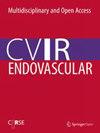
Between January 2017 and March 2022, UAE procedures were performed in 270 women for adenomyosis, some of whom also had fibroids. Eighteen women were identified with prior ablation failure (see Table 1): 15 with pure adenomyosis and 3 with coexisting fibroids. One woman was lost to follow-up; the outcomes of 17/18 (94.4%) were available for analysis, at a mean follow-up of 1.6 years post-UAE (median 2, range 0.6–3 years). Significant reductions in pain score (VAS 6.29), number of days in pain (2.6 days), symptom score (32.1/100), and significant improvement in QoL (39/100) were noted (Table 2). For the 8 women who still had HMB post-ablation, 7 (87.5%) saw significant improvement. Overall, 15/17 patients (88.2%) were “Satisfied” or “Very Satisfied” with the outcome of the UAE procedure (Fig. 1). Only 1 (5.9%) woman required a hysterectomy. No other women required further intervention such as laparoscopy for residual pain/endometriosis. No women reported menopause. No immediate or long-term complications were noted in this audit. Thirteen women (76.5%) attended follow-up imaging (Fig. 2). Significant uterine volume reduction and JZ thickness reduction were noted (Table 2).
a Results: Menstrual bleeding Post UAE. b Results: Overall outcome
Full size imageFig. 2
MRI of a 50-year-old woman who had endometrial ablation 10 months ago but was still suffering from heavy menstrual bleeding and severe dysmenorrhea. Following UAE, she had regular periods with lightest-ever bleeding and a reduction of pain score from 10 to 1. Sagittal T2 MRI pre- and post-embolisation demonstrated a reduction of uterine volume from 210 to 97 mL, reduction of junctional zone from 21 to 14 mm, less bulging globular appearance, and marked reduction of myometrial cystic spaces (ectopic endometrial tissue)
Full size image
The woman who failed UAE requiring subsequent hysterectomy had pure diffuse adenomyosis and scored the smallest uterine volume (62 mL) of the study cohort. Her angiography showed low uterine vascularity and bilateral small uterine arteries, which were pretreated with 100 µg of glycerol trinitrate on each side, prior to embolisation with nsPVA (Cook 200).
This study has shown that UAE can be an effective treatment for post-ablation adenomyosis, with significant improvement in pain and residual HMB. Overall patient satisfaction is 88.2%, and 94.1% were able to avoid a hysterectomy. The results from this post-ablation failure cohort compare favourably with previously reported overall UAE outcomes for adenomyosis [3, 4]. UAE as a non-targeted particle embolisation causes global ischemia of uterus. We postulate that normal myometrium can recover and remains viable due to numerous underlying dormant collateral vessels that can be recruited; abnormal tissue like adenomyosis does not have spare vessels to recruit and will undergo irreversible ischaemic infarction.
The question of whether EA is appropriate to treat adenomyosis should be raised. Depth of involvement of adenomyosis has been shown to be associated with endometrial ablation failure [8]. Deep adenomyosis (> 2.5 mm) is present in a significant number of women who underwent hysterectomy after failed endometrial ablation [2]. EA devices are designed to cause thermal destruction of 4–6 mm depth of tissue to the basalis level [9]. MRI diagnosis of adenomyosis requires junctional zone thickness of 12 mm or more [5]. Therefore, if the diagnosis of adenomyosis is established based on MRI criteria, there is a high chance that endometrial ablation might fail. We strongly argue that if adenomyosis is established on imaging, UAE should be offered to women as an alternative to hysterectomy, as many case series has demonstrated the safety and effectiveness of UAE for adenomyosis [3, 4]. Previous studies suggest that ablation either activates surviving endometrial tissue to penetrate the myometrium, causing adenomyosis, or activates embedded ectopic endometrial glands to grow deeper into the myometrium, resulting in deeper adenomyosis [8]. This might explain dysmenorrhea as a main clinical feature of EA failure that requires further intervention. Women with dysmenorrhea might have endometriosis and/or adenomyosis and are therefore at risk of persistent pelvic pain after endometrial ablation, which treats neither of the two underlying conditions. The presence of pre-existing dysmenorrhea is the most strongly correlated risk factor for receiving a surgical reintervention such as hysterectomy [1]. Women’s health practitioners should be aware that failure to correctly diagnose adenomyosis might result in the inadvertent use of ablation, leading to further intervention. Improved diagnostic accuracy of adenomyosis may reduce the number of women undergoing inappropriate ablation. This might require wider use of MRI, which has a higher sensitivity and specificity than ultrasound in diagnosing adenomyosis [10]. This is a small retrospective cohort study. The average follow-up of 1.6 years remains short, and the longer-term hysterectomy rate is yet to be defined by future studies. It is not known if the adenomyosis was present prior to EA or developed subsequent to EA. There is no pathological proof of the underlying pathology being treated by UAE. Future studies could be designed to use MRI to document the absence of adenomyosis prior to EA and see if there is a reduction in EA failure rate.
UAE is safe and effective in managing women who failed endometrial ablation, with significant improvement in dysmenorrhea and heavy menstrual bleeding. Most women were able to avoid hysterectomy following UAE for ablation failure.
Data is available for review upon request.
Beelen PP, Reinders WIM, Scheepers CFWM, Herman JM, Geomini PMA, Van Kuijk YMCM, Bongers MY. Prognostic factors for the failure of endometrial ablation: a systematic review and meta-analysis. Obstet Gynecol. 2019;134(6):1269–81.
Article PubMed Google Scholar
Mengerink BB, van der Wurff AAM, ter Haar JF, van Rooij IA, Pijnenborg JMA. Effect of undiagnosed deep adenomyosis after failed novasure endometrial ablation. J Minim Invasive Gynecol. 2015;22:239–44.
Article PubMed Google Scholar
de Bruijn AM, Smink M, Lohle PNM, Huirne JAF, Twisk JWR, Wong C, Schoonmade L, Hehenkamp WJK. Uterine artery embolization for the treatment of adenomyosis: a systematic review and meta-analysis. J Vasc Interv Radiol. 2017;28:1629–42.
Article PubMed Google Scholar
Liang E, Brown B, Rachinski M. A clinical audit on the efficacy and safety of uterine artery embolisation for symptomatic adenomyosis: results in 117 women. Aust N Z J Obstet Gynaecol. 2018;58:454–9.
Article PubMed Google Scholar
Agostinho L, Cruz R, Osório F, Alves J, Setúbal A, Guerra A. MRI for adenomyosis: a pictorial review. Insights Imaging. 2017. https://doi.org/10.1007/s13244-017-0576-z.
Article PubMed PubMed Central Google Scholar
Kim MD, Kim YM, Kim HC, Cho JH, Kang HG, Lee C, Kim HJ, Lee JT. Uterine artery embolization for symptomatic adenomyosis: a new technical development of the 1-2-3 protocol and predictive factors of MR imaging affecting outcomes. J Vasc Interv Radiol. 2011;22(4):497–502.
Article PubMed Google Scholar
Spies JB, Coyne K, Guaou Guaou N, et al. The UFS-QOL, a new disease-specific symptom and health-related quality of life questionnaire for leiomyomata. Obstet Gynecol. 2002;99(2):290–300.
PubMed Google Scholar
McCausland AM, McCausland VM. Depth of endometrial penetration in adenomyosis helps determine outcome of rollerball ablation. Am J Obstet Gynecol. 1996;174:1786–94.
Article CAS PubMed Google Scholar
Daub CA, Sepmeyer JA, Hathuc V, Sakala MD, Caserta MP, Clingan MJ, Hosseinzadeh K. Endometrial ablation: normal imaging appearance and delayed complications. Am J Roentgenol. 2015;205(4):W451–60.
Article Google Scholar
Champaneria R, Abedin P, Daniels J, Balogun M, Khan KS. Ultrasound scan and magnetic resonance imaging for the diagnosis of adenomyosis: systematic review comparing test accuracy. Acta Obstet Gynecol Scand. 2010;89(11):1374–84.
Article PubMed Google Scholar
Download references
No special acknowledgements.
There was no financial support from outside organisation.
Authors and Affiliations
Sydney Fibroid Clinic, Sydney, Australia
Eisen Liang, Razeen Parvez & Bevan Brown
Gosford Hospital, Gosford, NSW, Australia
Sylvia Ng
Authors
Eisen LiangView author publications
You can also search for this author in PubMedGoogle Scholar
Razeen ParvezView author publications
You can also search for this author in PubMedGoogle Scholar
Sylvia NgView author publications
You can also search for this author in PubMedGoogle Scholar
Bevan BrownView author publications
You can also search for this author in PubMedGoogle Scholar
Contributions
Authors’ contribution are as follows: Eisen Liang’s role: design concept, ethics submission data collection, literature review, drafting of paper, submission. Razeen Parvez’s role: data collection, data analysis, literature search, ethics submission. Sylvia Ng’s role: data analysis, literature search, drafting / formatting/ referencing, Bevan Brown’s role: design concept, literature review, review of draft and editing.
Authors’ information
Eisen Liang: Interventional Radiologist.
Razeen Parvez: Research Assistant, Medical student.
Sylvia Ng: Research Assistant, Radiology Trainee.
Bevan Brown: Gynaecologist.
Corresponding author
Correspondence to Eisen Liang.
Ethics approval and consent to participate
Informed consent was obtained from all individual participants involved in the study.
This study was approved by the Adventist HealthCare Limited Human Research Ethics Committee (HREC 2022–028).
Consent for publication
We consent for publication in CVIR Endovascular.
Competing interests
There is no conflict of interest identified.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Material 1.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Reprints and permissions
Cite this article
Liang, E., Parvez, R., Ng, S. et al. Uterine artery embolisation for adenomyosis in women who failed prior endometrial ablation. CVIR Endovasc7, 59 (2024). https://doi.org/10.1186/s42155-024-00471-5
Download citation
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s42155-024-00471-5
Share this article
Anyone you share the following link with will be able to read this content:
Sorry, a shareable link is not currently available for this article.
Provided by the Springer Nature SharedIt content-sharing initiative
子宫动脉栓塞治疗症状性腺肌症的有效性和安全性临床审核:117 名妇女的结果。Aust N Z J Obstet Gynaecol.2018;58:454-9.Article PubMed Google Scholar Agostinho L, Cruz R, Osório F, Alves J, Setúbal A, Guerra A. MRI for adenomyosis: a pictorial review.Insights Imaging.https://doi.org/10.1007/s13244-017-0576-z.Article PubMed PubMed Central Google Scholar Kim MD, Kim YM, Kim HC, Cho JH, Kang HG, Lee C, Kim HJ, Lee JT.子宫动脉栓塞治疗无症状子宫腺肌症:1-2-3方案的新技术发展和影响结果的磁共振成像预测因素。J Vasc Interv Radiol.2011; 22(4):497-502.Article PubMed Google Scholar Spies JB, Coyne K, Guaou Guaou N, et al. The UFS-QOL, a new disease-specific symptom and health-related quality of life questionnaire for leiomyomata.Obstet Gynecol.2002;99(2):290-300.PubMed Google Scholar McCausland AM, McCausland VM.子宫腺肌症的子宫内膜穿透深度有助于确定滚珠消融术的结果。Am J Obstet Gynecol.1996;174:1786-94.Article CAS PubMed Google Scholar Daub CA, Sepmeyer JA, Hathuc V, Sakala MD, Caserta MP, Clingan MJ, Hosseinzadeh K. Endometrial ablation: normal imaging appearance and delayed complications.Am J Roentgenol.2015;205(4):W451-60.Article Google Scholar Champaneria R, Abedin P, Daniels J, Balogun M, Khan KS.超声扫描和磁共振成像诊断子宫腺肌症:比较检测准确性的系统综述。Acta Obstet Gynecol Scand.2010;89(11):1374-84.Article PubMed Google Scholar Download references无特别鸣谢。作者和单位悉尼纤维瘤诊所,澳大利亚悉尼Eisen Liang, Razeen Parvez &;Bevan BrownGosford Hospital, Gosford, NSW, AustraliaSylvia Ng作者Eisen Liang查看作者发表的论文您也可以在PubMed Google Scholar中搜索该作者Razeen Parvez查看作者发表的论文您也可以在PubMed Google Scholar中搜索该作者Sylvia Ng查看作者发表的论文您也可以在PubMed Google Scholar中搜索该作者Bevan Brown查看作者发表的论文您也可以在PubMed Google Scholar中搜索该作者作者贡献作者的贡献如下:Eisen Liang 的职责:设计概念、伦理提交、数据收集、文献综述、论文起草、提交。Razeen Parvez 的职责:数据收集、数据分析、文献检索、伦理呈文。Sylvia Ng 的职责:数据分析、文献检索、起草/格式化/参考文献;Bevan Brown 的职责:设计概念、文献综述、审稿和编辑:研究助理,医科学生:Sylvia Ng:研究助理,放射科实习生:伦理批准和参与同意本研究获得了所有参与者的知情同意。本研究获得了基督复临安息日会医疗保健有限公司人类研究伦理委员会(HREC 2022-028)的批准。同意发表我们同意在《CVIR Endovascular》上发表。出版商注释Springer Nature对已出版地图中的管辖权主张和机构隶属关系保持中立。补充材料1.开放获取本文采用知识共享署名 4.0 国际许可协议进行许可,该协议允许以任何媒介或格式使用、共享、改编、分发和复制,只要您适当注明原作者和来源,提供知识共享许可协议的链接,并说明是否进行了更改。本文中的图片或其他第三方材料均包含在文章的知识共享许可协议中,除非在材料的署名栏中另有说明。如果材料未包含在文章的知识共享许可协议中,且您打算使用的材料不符合法律规定或超出许可使用范围,则您需要直接从版权所有者处获得许可。如需查看该许可的副本,请访问 http://creativecommons.org/licenses/by/4.0/.Reprints and permissionsCite this articleLiang, E., Parvez, R., Ng, S. et al. Uterine artery embolisation for adenomyosis in women who failed prior endometrial ablation.https://doi.org/10.1186/s42155-024-00471-5Download citationReceived:08 June 2024Accepted:10 July 2024Published: 27 July 2024DOI: https://doi.org/10.1186/s42155-024-00471-5Share this articleAnyone you share the following link with will be able to read this content:Get shareable linkSorry, a shareable link is not currently available for this article.Copy to clipboard Provided by the Springer Nature SharedIt content-sharing initiative.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
