A Regional Survey of Attitudes and Experiences in Determining When to Prescribe Intranasal Naloxone for Patients Seen in Palliative Care Clinics in the United States of America.
Sean Marks, Divya Patel, Rabia Amjad, April Dawson, Rebekah J Walker, Drew A Rosielle
{"title":"A Regional Survey of Attitudes and Experiences in Determining When to Prescribe Intranasal Naloxone for Patients Seen in Palliative Care Clinics in the United States of America.","authors":"Sean Marks, Divya Patel, Rabia Amjad, April Dawson, Rebekah J Walker, Drew A Rosielle","doi":"10.1089/pmr.2024.0027","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Published guidelines that help clinicians identify patients who would benefit from the co-prescription of intranasal naloxone (IN) exclude \"palliative care patients.\" In the absence of clear care standards, palliative care (PC) clinicians may experience uncertainty in how to approach IN co-prescriptions.</p><p><strong>Objective: </strong>Explore the attitudes of PC clinicians in the United States of America who work at regional health care institutions regarding IN prescriptions for patients they prescribe opioids for.</p><p><strong>Methods: </strong>An 18-question electronic survey was distributed to PC clinicians that practice at institutions in Wisconsin or Minnesota with at least 10 other PC clinicians between February and May 2023. The survey explored clinical scenarios in which respondents would and would not prescribe IN.</p><p><strong>Results: </strong>Fifty-six PC clinicians responded to the survey-response rate 41%. Most respondents (90.9%) did not feel IN prescriptions should be reserved for patients with a full code status; 67.9% of respondents felt that IN prescriptions are reasonable for certain patients with a terminal illness and comfort goals of care. Neither prognosis, duration of opioid therapy, nor dose of opioid therapy were significant factors in determining whether most respondents prescribed IN for their patients. Most respondents (81.8%) felt clinician counseling and patient consent were essential before prescribing IN.</p><p><strong>Conclusion: </strong>Most PC clinicians in our survey felt that IN prescriptions can be appropriate for patients they prescribe opioids for. Bystander safety was an emerging rationale for why respondents chose to prescribe IN for their patients. Despite public health efforts to make IN more freely available, most respondents felt clinician counseling was essential before prescribing IN for their patients.</p>","PeriodicalId":74394,"journal":{"name":"Palliative medicine reports","volume":"5 1","pages":"286-292"},"PeriodicalIF":1.3000,"publicationDate":"2024-07-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11271067/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Palliative medicine reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/pmr.2024.0027","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Published guidelines that help clinicians identify patients who would benefit from the co-prescription of intranasal naloxone (IN) exclude "palliative care patients." In the absence of clear care standards, palliative care (PC) clinicians may experience uncertainty in how to approach IN co-prescriptions.
Objective: Explore the attitudes of PC clinicians in the United States of America who work at regional health care institutions regarding IN prescriptions for patients they prescribe opioids for.
Methods: An 18-question electronic survey was distributed to PC clinicians that practice at institutions in Wisconsin or Minnesota with at least 10 other PC clinicians between February and May 2023. The survey explored clinical scenarios in which respondents would and would not prescribe IN.
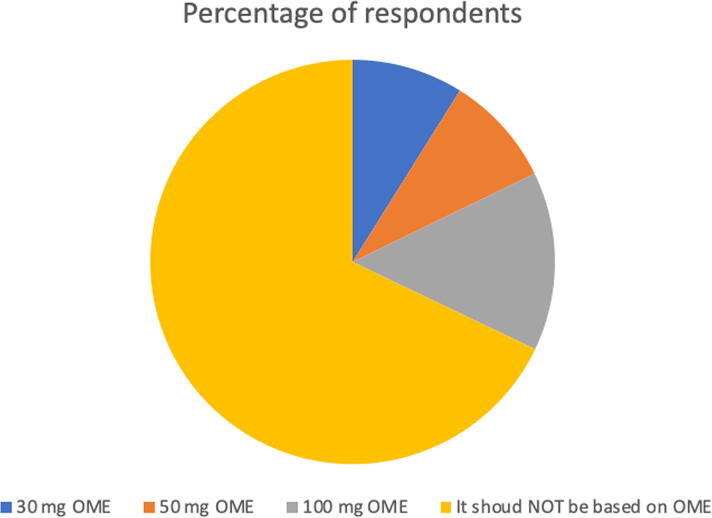
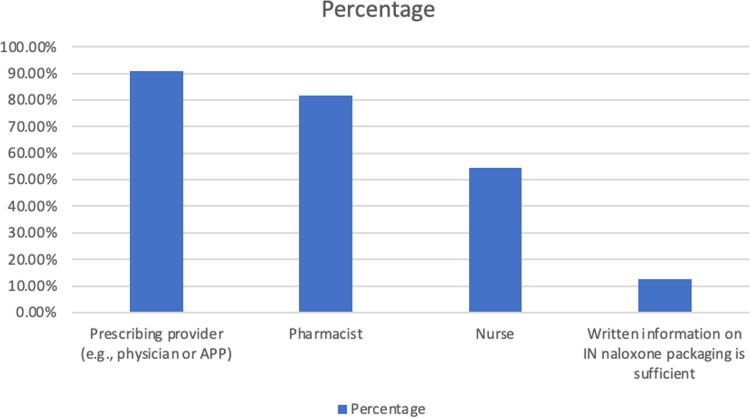
Results: Fifty-six PC clinicians responded to the survey-response rate 41%. Most respondents (90.9%) did not feel IN prescriptions should be reserved for patients with a full code status; 67.9% of respondents felt that IN prescriptions are reasonable for certain patients with a terminal illness and comfort goals of care. Neither prognosis, duration of opioid therapy, nor dose of opioid therapy were significant factors in determining whether most respondents prescribed IN for their patients. Most respondents (81.8%) felt clinician counseling and patient consent were essential before prescribing IN.
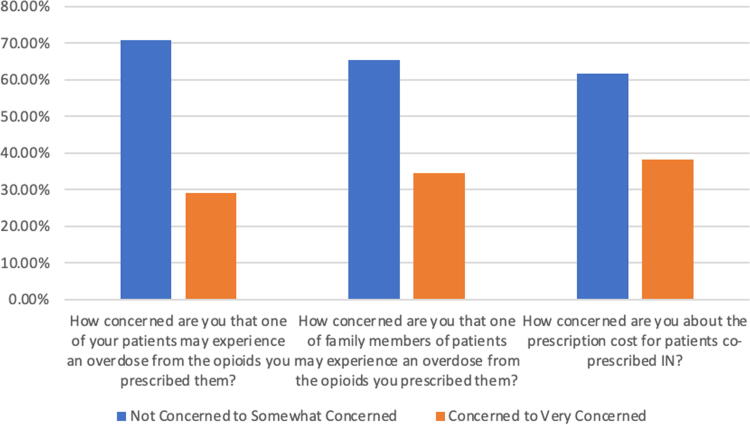
Conclusion: Most PC clinicians in our survey felt that IN prescriptions can be appropriate for patients they prescribe opioids for. Bystander safety was an emerging rationale for why respondents chose to prescribe IN for their patients. Despite public health efforts to make IN more freely available, most respondents felt clinician counseling was essential before prescribing IN for their patients.
背景:已发布的帮助临床医生识别可从鼻内纳洛酮(IN)联合处方中获益的患者的指南将 "姑息治疗患者 "排除在外。由于缺乏明确的护理标准,姑息治疗(PC)临床医生在如何处理纳洛酮联合处方时可能会遇到不确定性:探讨美国地区医疗机构中的姑息治疗临床医生对其为阿片类药物患者开具 IN 处方的态度:在 2023 年 2 月至 5 月期间,我们向在威斯康星州或明尼苏达州的医疗机构执业且至少有 10 名其他 PC 临床医生的 PC 临床医生发放了一份包含 18 个问题的电子调查问卷。调查探讨了受访者会或不会开具 IN 的临床情景:56 名 PC 临床医生对调查做出了回复,回复率为 41%。大多数受访者(90.9%)认为,IN 处方不应仅限于完全代码状态的患者;67.9% 的受访者认为,IN 处方对于某些身患绝症并有舒适护理目标的患者是合理的。预后、阿片类药物治疗的持续时间和剂量都不是决定大多数受访者是否为患者开具 IN 处方的重要因素。大多数受访者(81.8%)认为,在开具 IN 处方之前,临床医生的咨询和患者的同意至关重要:结论:在我们的调查中,大多数 PC 临床医生认为,IN 处方对于他们开阿片类药物处方的患者是合适的。旁观者安全是受访者选择为患者开 IN 处方的一个新理由。尽管公共卫生机构努力使 IN 更容易获得,但大多数受访者认为,在为患者开具 IN 处方之前,临床医生的咨询是必不可少的。



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
