Auke T. Bergeman, Said Nourdine, Alberto Piubello, Zahara Salim, Sofie M. Braet, Abdallah Baco, Silahi H. Grillone, Rian Snijders, Carolien Hoof, Achilleas Tsoumanis, Harry van Loen, Younoussa Assoumani, Aboubacar Mzembaba, Nimer Ortuño-Gutiérrez, Epco Hasker, Christian van der Werf, Bouke C. de Jong
{"title":"Feasibility and accuracy of mobile QT interval monitoring strategies in bedaquiline-enhanced prophylactic leprosy treatment","authors":"Auke T. Bergeman, Said Nourdine, Alberto Piubello, Zahara Salim, Sofie M. Braet, Abdallah Baco, Silahi H. Grillone, Rian Snijders, Carolien Hoof, Achilleas Tsoumanis, Harry van Loen, Younoussa Assoumani, Aboubacar Mzembaba, Nimer Ortuño-Gutiérrez, Epco Hasker, Christian van der Werf, Bouke C. de Jong","doi":"10.1111/cts.13861","DOIUrl":null,"url":null,"abstract":"<p>Some anti-mycobacterial drugs are known to cause QT interval prolongation, potentially leading to life-threatening ventricular arrhythmia. However, the highest leprosy and tuberculosis burden occurs in settings where electrocardiographic monitoring is challenging. The feasibility and accuracy of alternative strategies, such as the use of automated measurements or a mobile electrocardiogram (mECG) device, have not been evaluated in this context. As part of the phase II randomized controlled BE-PEOPLE trial evaluating the safety of bedaquiline-enhanced post-exposure prophylaxis (bedaquiline and rifampicin, BE-PEP, versus rifampicin, SDR-PEP) for leprosy, all participants had corrected QT intervals (QTc) measured at baseline and on the day after receiving post-exposure prophylaxis. The accuracy of mECG measurements as well as automated 12L-ECG measurements was evaluated. In total, 635 mECGs from 323 participants were recorded, of which 616 (97%) were of sufficient quality for QTc measurement. Mean manually read QTc on 12L-ECG and mECG were 394 ± 19 and 385 ± 18 ms, respectively (<i>p</i> < 0.001), with a strong correlation (<i>r</i> = 0.793). The mean absolute QTc difference between both modalities was 11 ± 10 ms. Mean manual and automated 12L-ECG QTc were 394 ± 19 and 409 ± 19 ms, respectively (<i>n</i> = 636; <i>p</i> < 0.001), corresponding to moderate agreement (<i>r</i> = 0.655). The use of a mECG device for QT interval monitoring was feasible and yielded a median absolute QTc error of 8 ms. Automated QTc measurements were less accurate, yielding longer QTc intervals.</p>","PeriodicalId":50610,"journal":{"name":"Cts-Clinical and Translational Science","volume":"17 8","pages":""},"PeriodicalIF":2.8000,"publicationDate":"2024-07-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11286973/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cts-Clinical and Translational Science","FirstCategoryId":"3","ListUrlMain":"https://ascpt.onlinelibrary.wiley.com/doi/10.1111/cts.13861","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 0
Abstract
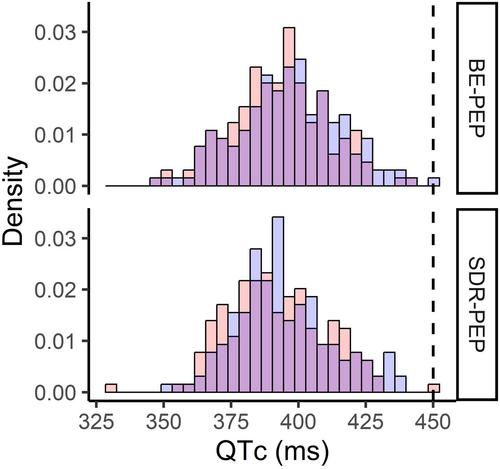
Some anti-mycobacterial drugs are known to cause QT interval prolongation, potentially leading to life-threatening ventricular arrhythmia. However, the highest leprosy and tuberculosis burden occurs in settings where electrocardiographic monitoring is challenging. The feasibility and accuracy of alternative strategies, such as the use of automated measurements or a mobile electrocardiogram (mECG) device, have not been evaluated in this context. As part of the phase II randomized controlled BE-PEOPLE trial evaluating the safety of bedaquiline-enhanced post-exposure prophylaxis (bedaquiline and rifampicin, BE-PEP, versus rifampicin, SDR-PEP) for leprosy, all participants had corrected QT intervals (QTc) measured at baseline and on the day after receiving post-exposure prophylaxis. The accuracy of mECG measurements as well as automated 12L-ECG measurements was evaluated. In total, 635 mECGs from 323 participants were recorded, of which 616 (97%) were of sufficient quality for QTc measurement. Mean manually read QTc on 12L-ECG and mECG were 394 ± 19 and 385 ± 18 ms, respectively (p < 0.001), with a strong correlation (r = 0.793). The mean absolute QTc difference between both modalities was 11 ± 10 ms. Mean manual and automated 12L-ECG QTc were 394 ± 19 and 409 ± 19 ms, respectively (n = 636; p < 0.001), corresponding to moderate agreement (r = 0.655). The use of a mECG device for QT interval monitoring was feasible and yielded a median absolute QTc error of 8 ms. Automated QTc measurements were less accurate, yielding longer QTc intervals.
期刊介绍:
Clinical and Translational Science (CTS), an official journal of the American Society for Clinical Pharmacology and Therapeutics, highlights original translational medicine research that helps bridge laboratory discoveries with the diagnosis and treatment of human disease. Translational medicine is a multi-faceted discipline with a focus on translational therapeutics. In a broad sense, translational medicine bridges across the discovery, development, regulation, and utilization spectrum. Research may appear as Full Articles, Brief Reports, Commentaries, Phase Forwards (clinical trials), Reviews, or Tutorials. CTS also includes invited didactic content that covers the connections between clinical pharmacology and translational medicine. Best-in-class methodologies and best practices are also welcomed as Tutorials. These additional features provide context for research articles and facilitate understanding for a wide array of individuals interested in clinical and translational science. CTS welcomes high quality, scientifically sound, original manuscripts focused on clinical pharmacology and translational science, including animal, in vitro, in silico, and clinical studies supporting the breadth of drug discovery, development, regulation and clinical use of both traditional drugs and innovative modalities.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
