{"title":"Unique endoscopic features of primary biliary diffuse large B-cell lymphoma: A case report with literature review (with video)","authors":"Tomoya Nakamura, Yoshiharu Masaki, Naohiro Kameyama, Yujiro Kawakami, Keisuke Ishigami, Yumemi Takada, Shuji Satoh, Taro Sugawara, Shintaro Sugita, Hiroshi Nakase","doi":"10.1002/deo2.414","DOIUrl":null,"url":null,"abstract":"<p>A 67-year-old man visited our hospital complaining of dark-colored urine and upper abdominal pain. Magnetic resonance cholangiopancreatography showed stricture of the distal bile duct, and contrast-enhanced computed tomography showed irregular thickening of the distal bile duct wall. However, no enlarged lymph nodes, pancreatic tumors, or other neoplastic lesions were apparent around the bile duct. Endoscopic ultrasonography and intraductal ultrasonography showed irregular thickening of the inner hypoechoic layer without the disappearance of the innermost thin hyperechoic layer. On the basis of these findings, we considered that the bile duct lesion was of non-epithelial origin. Thus, we repeatedly performed bile duct biopsies from the same site under fluoroscopy to obtain a sample of the submucosal tissue. The pathological diagnosis was diffuse large B-cell lymphoma, and the patient received systemic chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). After six courses of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone, positron emission tomography-computed tomography showed the disappearance of 18-fluorodeoxyglucose uptake in the bile duct and endoscopic retrograde cholangiography showed improvement of the bile duct stricture. Endoscopic findings and repeated biopsies were useful in making the diagnosis of primary biliary diffuse large B-cell lymphoma.</p>","PeriodicalId":93973,"journal":{"name":"DEN open","volume":"5 1","pages":""},"PeriodicalIF":1.5000,"publicationDate":"2024-07-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11284119/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"DEN open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/deo2.414","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
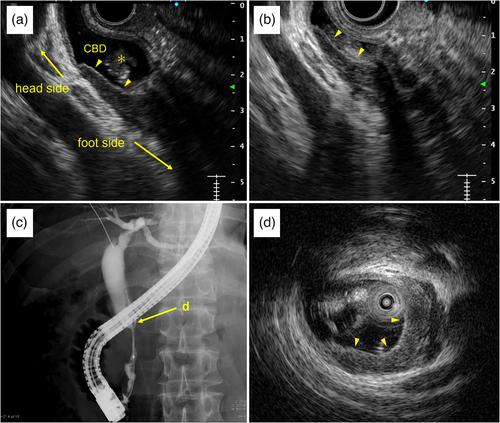
A 67-year-old man visited our hospital complaining of dark-colored urine and upper abdominal pain. Magnetic resonance cholangiopancreatography showed stricture of the distal bile duct, and contrast-enhanced computed tomography showed irregular thickening of the distal bile duct wall. However, no enlarged lymph nodes, pancreatic tumors, or other neoplastic lesions were apparent around the bile duct. Endoscopic ultrasonography and intraductal ultrasonography showed irregular thickening of the inner hypoechoic layer without the disappearance of the innermost thin hyperechoic layer. On the basis of these findings, we considered that the bile duct lesion was of non-epithelial origin. Thus, we repeatedly performed bile duct biopsies from the same site under fluoroscopy to obtain a sample of the submucosal tissue. The pathological diagnosis was diffuse large B-cell lymphoma, and the patient received systemic chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). After six courses of rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone, positron emission tomography-computed tomography showed the disappearance of 18-fluorodeoxyglucose uptake in the bile duct and endoscopic retrograde cholangiography showed improvement of the bile duct stricture. Endoscopic findings and repeated biopsies were useful in making the diagnosis of primary biliary diffuse large B-cell lymphoma.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
