Pol Olivas , Alexandre Soler-Perromat , Luis Tellez , José Antonio Carrión , Edilmar Alvarado-Tapias , José Ferrusquía-Acosta , Sabela Lens , Antonio Guerrero , Ángeles Falgà , Pamela Vizcarra , Lara Orts , Valeria Perez-Campuzano , Sarah Shalaby , Sonia Torres , Anna Baiges , Fanny Turon , Juan Carlos García-Pagán , Ángeles García-Criado , Virginia Hernández-Gea
{"title":"Persistent varices in cured patients: Understanding the role of hepatic venous pressure gradient","authors":"Pol Olivas , Alexandre Soler-Perromat , Luis Tellez , José Antonio Carrión , Edilmar Alvarado-Tapias , José Ferrusquía-Acosta , Sabela Lens , Antonio Guerrero , Ángeles Falgà , Pamela Vizcarra , Lara Orts , Valeria Perez-Campuzano , Sarah Shalaby , Sonia Torres , Anna Baiges , Fanny Turon , Juan Carlos García-Pagán , Ángeles García-Criado , Virginia Hernández-Gea","doi":"10.1016/j.jhepr.2024.101170","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><div>Etiologic factor removal (ER) drives recompensation and improves portal hypertension in cirrhosis. Esophageal varices (EV) and portosystemic shunts (PSS) have been found in patients despite hepatic venous pressure gradient (HVPG) dropping below 10 mmHg after ER, questioning HVPG accuracy in reflecting true portal pressure in the setting of ER. We aim to evaluate the correlation of HVPG with direct portal pressure (DPP) in patients with persistence of EV after ER despite HVPG <10 mmHg.</div></div><div><h3>Methods</h3><div>This is a bicentric ‘proof of concept’ study evaluating HVPG and ultrasound-guided percutaneous DPP in patients with HCV or alcohol-related cirrhosis with persistent varices and HVPG <10 mmHg after at least 5 years of ER.</div></div><div><h3>Results</h3><div>Seven patients with HCV and three with alcohol-related cirrhosis with persistent varices and HVPG <10 mmHg after at least 5 years of ER were included. At evaluation, all patients had a patent portal vein and were compensated. The median platelet count was 129.5 (IQR 95–145) × 10<sup>9</sup>/ml, and the median liver stiffness measurement was 16.15 (IQR 14.4–22.3) kPa. In five patients, EV remained the same size (two large and three small), and five downsized to small after ER. Wedge hepatic vein pressure (median 19 [IQR 16.5–20] mmHg) and portal pressure (median 18 [IQR 15–19.5] mmHg) had an excellent correlation (R = 0.93, <em>p</em> <0.0001). Portal pressure gradient (PPG) confirmed the absence of clinically significant portal hypertension as identified by HVPG across all the patients.</div></div><div><h3>Conclusions</h3><div>HVPG accurately reflects PPG in the context of HCV and alcohol-related cirrhosis regression. After ER, EV may persist despite HVPG <10 mmHg. The benefit of prophylaxis in patients with EV and HVPG <10 mmHg is unknown. Future studies with clinical endpoints are needed to validate our findings.</div></div><div><h3>Impact and implications:</h3><div>Despite a favorable evolution after the removal of the etiologic factor, varices persist in some patients, and there is a lack of concise guidelines for the evaluation and management of portal hypertension in this population. Our research underscores the persistence of varices in the absence of clinically significant portal hypertension and significantly demonstrates the accuracy of hepatic venous pressure gradient (HVPG) in reflecting portal vein pressure in this specific patient group. These findings emphasize the crucial role of HVPG in the assessment of portal hypertension after etiologic factor removal and lay the groundwork for further investigation into clinical outcomes and the necessity of non-selective beta-blockers in individuals with persistent varices after the removal of etiologic factor.</div></div>","PeriodicalId":14764,"journal":{"name":"JHEP Reports","volume":"6 10","pages":"Article 101170"},"PeriodicalIF":7.5000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JHEP Reports","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589555924001745","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background & Aims
Etiologic factor removal (ER) drives recompensation and improves portal hypertension in cirrhosis. Esophageal varices (EV) and portosystemic shunts (PSS) have been found in patients despite hepatic venous pressure gradient (HVPG) dropping below 10 mmHg after ER, questioning HVPG accuracy in reflecting true portal pressure in the setting of ER. We aim to evaluate the correlation of HVPG with direct portal pressure (DPP) in patients with persistence of EV after ER despite HVPG <10 mmHg.
Methods
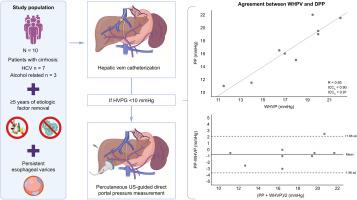
This is a bicentric ‘proof of concept’ study evaluating HVPG and ultrasound-guided percutaneous DPP in patients with HCV or alcohol-related cirrhosis with persistent varices and HVPG <10 mmHg after at least 5 years of ER.
Results
Seven patients with HCV and three with alcohol-related cirrhosis with persistent varices and HVPG <10 mmHg after at least 5 years of ER were included. At evaluation, all patients had a patent portal vein and were compensated. The median platelet count was 129.5 (IQR 95–145) × 109/ml, and the median liver stiffness measurement was 16.15 (IQR 14.4–22.3) kPa. In five patients, EV remained the same size (two large and three small), and five downsized to small after ER. Wedge hepatic vein pressure (median 19 [IQR 16.5–20] mmHg) and portal pressure (median 18 [IQR 15–19.5] mmHg) had an excellent correlation (R = 0.93, p <0.0001). Portal pressure gradient (PPG) confirmed the absence of clinically significant portal hypertension as identified by HVPG across all the patients.
Conclusions
HVPG accurately reflects PPG in the context of HCV and alcohol-related cirrhosis regression. After ER, EV may persist despite HVPG <10 mmHg. The benefit of prophylaxis in patients with EV and HVPG <10 mmHg is unknown. Future studies with clinical endpoints are needed to validate our findings.
Impact and implications:
Despite a favorable evolution after the removal of the etiologic factor, varices persist in some patients, and there is a lack of concise guidelines for the evaluation and management of portal hypertension in this population. Our research underscores the persistence of varices in the absence of clinically significant portal hypertension and significantly demonstrates the accuracy of hepatic venous pressure gradient (HVPG) in reflecting portal vein pressure in this specific patient group. These findings emphasize the crucial role of HVPG in the assessment of portal hypertension after etiologic factor removal and lay the groundwork for further investigation into clinical outcomes and the necessity of non-selective beta-blockers in individuals with persistent varices after the removal of etiologic factor.
期刊介绍:
JHEP Reports is an open access journal that is affiliated with the European Association for the Study of the Liver (EASL). It serves as a companion journal to the highly respected Journal of Hepatology.
The primary objective of JHEP Reports is to publish original papers and reviews that contribute to the advancement of knowledge in the field of liver diseases. The journal covers a wide range of topics, including basic, translational, and clinical research. It also focuses on global issues in hepatology, with particular emphasis on areas such as clinical trials, novel diagnostics, precision medicine and therapeutics, cancer research, cellular and molecular studies, artificial intelligence, microbiome research, epidemiology, and cutting-edge technologies.
In summary, JHEP Reports is dedicated to promoting scientific discoveries and innovations in liver diseases through the publication of high-quality research papers and reviews covering various aspects of hepatology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
