Predischarge Peak Atrial Longitudinal Strain and Plasma N-terminal Pro-hormone Brain Natriuretic Peptide as a Predictor of Short-term Rehospitalization and Cardiovascular Mortality in Patients with Acute Heart Failure.
I Gusti Bagus Putu Suwarjana Kaler, Ida Bagus Rangga Wibhuti, I Nyoman Wiryawan, A A Wiradewi Lestari
{"title":"Predischarge Peak Atrial Longitudinal Strain and Plasma N-terminal Pro-hormone Brain Natriuretic Peptide as a Predictor of Short-term Rehospitalization and Cardiovascular Mortality in Patients with Acute Heart Failure.","authors":"I Gusti Bagus Putu Suwarjana Kaler, Ida Bagus Rangga Wibhuti, I Nyoman Wiryawan, A A Wiradewi Lestari","doi":"10.4103/jcecho.jcecho_70_23","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>The postacute heart failure (AHF) rehospitalization rate is attributed to persistent hemodynamic congestion despite clinical improvement. Peak atrial longitudinal strain (PALS), utilizing speckle tracking echocardiography technology, shows potential in post-AHF prognosis. Meanwhile, N-terminal pro-hormone brain natriuretic peptide (NT-proBNP) remains a known biomarker of intracardiac congestion.</p><p><strong>Aims: </strong>This study aimed to determine the relationship between predischarge PALS and NT-proBNP as predictors of major adverse cardiac event (MACE) in patients after AHF hospitalization.</p><p><strong>Settings and design: </strong>This study is a prospective cohort study, conducted in Prof. Dr. I G.N.G Ngoerah Hospital, Bali, Indonesia.</p><p><strong>Subjects and methods: </strong>The study included hospitalized AHF patients, collecting demographic data, comorbidities, therapies, and echocardiographic measures before discharge. Predischarge PALS and NT-proBNP were taken within 24 h before discharge. The main outcome was MACE, defined as rehospitalization and cardiovascular mortality within 90 days.</p><p><strong>Statistical analysis used: </strong>Comparative statistical analyses was done using independent <i>t</i>-test for continuous variables (Mann-Whitney <i>U</i> test for variables with abnormal distribution) and Chi-squared tests. Receiver operating characteristic (ROC) used in determining optimal threshold values of predischarge PALS and NT-proBNP as a predictor of MACE. Kaplan-Meier curves were employed to gauge event-free survival differences between these cohorts. Then, independent Cox regression was used to identify the predictors of MACE.</p><p><strong>Results: </strong>The study enrolled 67 patients with varying ejection fraction (EF) (16 - heart failure with preserved ejection fraction, 10 - heart failure with mildly reduced ejection fraction, and 41 - heart failure with reduced ejection fraction; mean age: 56.88 ± 14.57 years). Over the 90-day follow-up, 21 patients (31.3%) encountered MACE. Both PALS (area under the curve [AUC] 0.816) and NT-proBNP (AUC 0.856) before discharge served as predictors of MACE. There was no significant AUC difference between ROC curves (area difference: 0.039, <i>P</i> = 0.553). The regression model highlighted that PALS and NT-proBNP level before discharge acted as independent predictors of MACE, irrespective of EF, average E/e', or estimated predischarge pulmonary capillary wedge pressure.</p><p><strong>Conclusions: </strong>Predischarge PALS is comparable to NT-proBNP levels as independent predictors of short-term MACE after AHF hospitalization.</p>","PeriodicalId":15191,"journal":{"name":"Journal of Cardiovascular Echography","volume":"34 2","pages":"63-71"},"PeriodicalIF":1.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11288303/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular Echography","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jcecho.jcecho_70_23","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/6/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 0
Abstract
Context: The postacute heart failure (AHF) rehospitalization rate is attributed to persistent hemodynamic congestion despite clinical improvement. Peak atrial longitudinal strain (PALS), utilizing speckle tracking echocardiography technology, shows potential in post-AHF prognosis. Meanwhile, N-terminal pro-hormone brain natriuretic peptide (NT-proBNP) remains a known biomarker of intracardiac congestion.
Aims: This study aimed to determine the relationship between predischarge PALS and NT-proBNP as predictors of major adverse cardiac event (MACE) in patients after AHF hospitalization.
Settings and design: This study is a prospective cohort study, conducted in Prof. Dr. I G.N.G Ngoerah Hospital, Bali, Indonesia.
Subjects and methods: The study included hospitalized AHF patients, collecting demographic data, comorbidities, therapies, and echocardiographic measures before discharge. Predischarge PALS and NT-proBNP were taken within 24 h before discharge. The main outcome was MACE, defined as rehospitalization and cardiovascular mortality within 90 days.
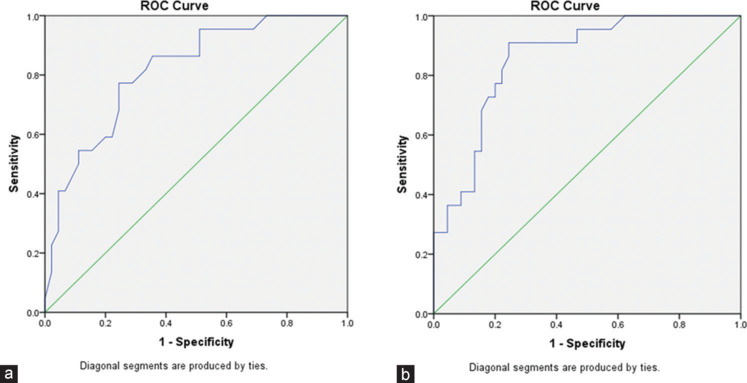
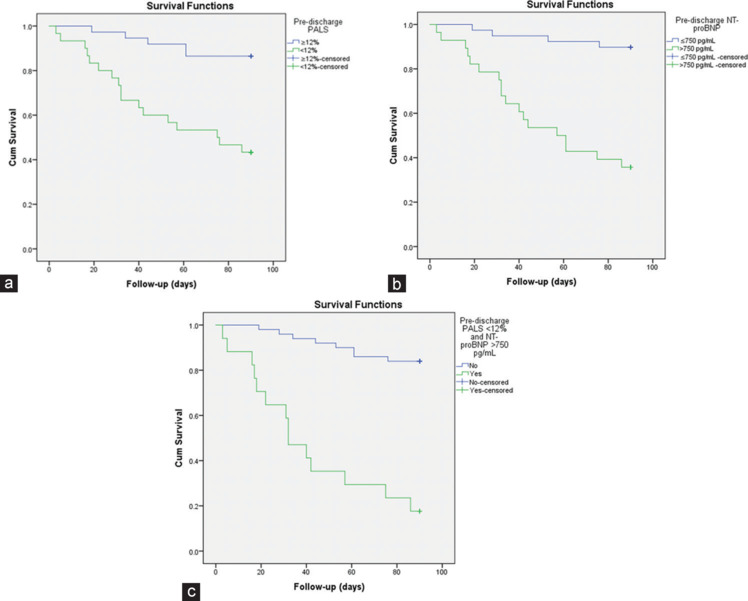
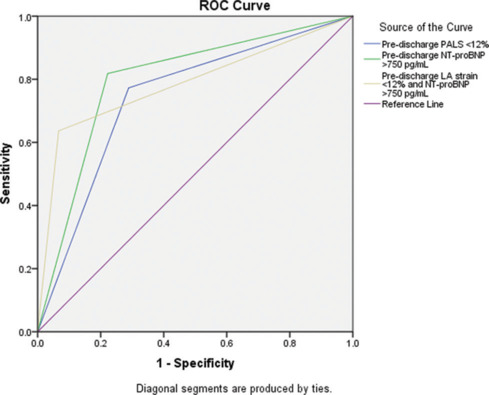
Statistical analysis used: Comparative statistical analyses was done using independent t-test for continuous variables (Mann-Whitney U test for variables with abnormal distribution) and Chi-squared tests. Receiver operating characteristic (ROC) used in determining optimal threshold values of predischarge PALS and NT-proBNP as a predictor of MACE. Kaplan-Meier curves were employed to gauge event-free survival differences between these cohorts. Then, independent Cox regression was used to identify the predictors of MACE.
Results: The study enrolled 67 patients with varying ejection fraction (EF) (16 - heart failure with preserved ejection fraction, 10 - heart failure with mildly reduced ejection fraction, and 41 - heart failure with reduced ejection fraction; mean age: 56.88 ± 14.57 years). Over the 90-day follow-up, 21 patients (31.3%) encountered MACE. Both PALS (area under the curve [AUC] 0.816) and NT-proBNP (AUC 0.856) before discharge served as predictors of MACE. There was no significant AUC difference between ROC curves (area difference: 0.039, P = 0.553). The regression model highlighted that PALS and NT-proBNP level before discharge acted as independent predictors of MACE, irrespective of EF, average E/e', or estimated predischarge pulmonary capillary wedge pressure.
Conclusions: Predischarge PALS is comparable to NT-proBNP levels as independent predictors of short-term MACE after AHF hospitalization.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
