Yuta Ichikawa, Nana Sakakibara, China Nagano, Yuta Inoki, Yu Tanaka, Chika Ueda, Hideaki Kitakado, Atsushi Kondo, Shingo Ishimori, Tomoko Horinouchi, Kazumoto Iijima, Kandai Nozu
{"title":"In steroid-resistant nephrotic syndrome that meets the strict definition, monogenic variants are less common than expected.","authors":"Yuta Ichikawa, Nana Sakakibara, China Nagano, Yuta Inoki, Yu Tanaka, Chika Ueda, Hideaki Kitakado, Atsushi Kondo, Shingo Ishimori, Tomoko Horinouchi, Kazumoto Iijima, Kandai Nozu","doi":"10.1007/s00467-024-06468-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In patients with steroid-resistant nephrotic syndrome (SRNS), the presence of monogenic variants influences therapeutic strategies. Large cohort studies reported the detection of monogenic variants in approximately 30% of patients with SRNS. However, these cohorts included many patients, such as those with symptomatic proteinuria, who did not meet the strict diagnostic criteria for pediatric nephrotic syndrome (NS). Therefore, we investigated the proportion of causative monogenic variants detected in patients who strictly met the diagnostic criteria of SRNS and explored their clinical characteristics.</p><p><strong>Methods: </strong>We examined pediatric SRNS cases with genetic analysis conducted in our hospital. Cases satisfying all of the following criteria were included: (1) age at onset 1-18 years, (2) serum albumin at onset ≤ 2.5 g/dl, (3) persistent heavy proteinuria, and (4) no complete remission after 4 weeks of steroid monotherapy.</p><p><strong>Results: </strong>The proportion of detected monogenic variants was 12% (22/185) among all patients. The proportion was only 7% (9/129) in patients with edema at disease onset compared with 38% (9/24) in those without (p < 0.0001). Monogenic variants were rare in patients with acute kidney injury associated with NS (1% (1/11)) or a history of complete remission (4% (2/51)).</p><p><strong>Conclusions: </strong>Our study revealed a monogenic cause in 12% of individuals with strictly defined SRNS, a much smaller proportion than previously reported. The presence or absence of edema at the onset was an important factor to distinguish SRNS with monogenic cause from SRNS without. Our results provide further evidence of the SRNS types attributable to monogenic causes.</p>","PeriodicalId":19735,"journal":{"name":"Pediatric Nephrology","volume":" ","pages":"3497-3503"},"PeriodicalIF":2.6000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11511720/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pediatric Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s00467-024-06468-5","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/2 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: In patients with steroid-resistant nephrotic syndrome (SRNS), the presence of monogenic variants influences therapeutic strategies. Large cohort studies reported the detection of monogenic variants in approximately 30% of patients with SRNS. However, these cohorts included many patients, such as those with symptomatic proteinuria, who did not meet the strict diagnostic criteria for pediatric nephrotic syndrome (NS). Therefore, we investigated the proportion of causative monogenic variants detected in patients who strictly met the diagnostic criteria of SRNS and explored their clinical characteristics.
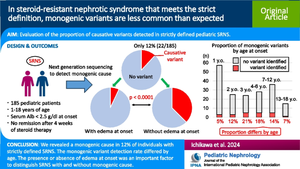
Methods: We examined pediatric SRNS cases with genetic analysis conducted in our hospital. Cases satisfying all of the following criteria were included: (1) age at onset 1-18 years, (2) serum albumin at onset ≤ 2.5 g/dl, (3) persistent heavy proteinuria, and (4) no complete remission after 4 weeks of steroid monotherapy.
Results: The proportion of detected monogenic variants was 12% (22/185) among all patients. The proportion was only 7% (9/129) in patients with edema at disease onset compared with 38% (9/24) in those without (p < 0.0001). Monogenic variants were rare in patients with acute kidney injury associated with NS (1% (1/11)) or a history of complete remission (4% (2/51)).
Conclusions: Our study revealed a monogenic cause in 12% of individuals with strictly defined SRNS, a much smaller proportion than previously reported. The presence or absence of edema at the onset was an important factor to distinguish SRNS with monogenic cause from SRNS without. Our results provide further evidence of the SRNS types attributable to monogenic causes.
期刊介绍:
International Pediatric Nephrology Association
Pediatric Nephrology publishes original clinical research related to acute and chronic diseases that affect renal function, blood pressure, and fluid and electrolyte disorders in children. Studies may involve medical, surgical, nutritional, physiologic, biochemical, genetic, pathologic or immunologic aspects of disease, imaging techniques or consequences of acute or chronic kidney disease. There are 12 issues per year that contain Editorial Commentaries, Reviews, Educational Reviews, Original Articles, Brief Reports, Rapid Communications, Clinical Quizzes, and Letters to the Editors.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
