Xin Ya See, Yu-Cheng Chang, Chun-Yu Peng, Shih-Syuan Wang, Kuan-Yu Chi, Cho-Hung Chiang, Cho-Han Chiang
{"title":"Rate of Sodium Correction and Osmotic Demyelination Syndrome in Severe Hyponatremia: A Meta-Analysis.","authors":"Xin Ya See, Yu-Cheng Chang, Chun-Yu Peng, Shih-Syuan Wang, Kuan-Yu Chi, Cho-Hung Chiang, Cho-Han Chiang","doi":"10.2478/jccm-2024-0030","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Current guidelines recommend limiting the rate of correction in patients with severe hyponatremia to avoid severe neurologic complications such as osmotic demyelination syndrome (ODS). However, published data have been conflicting. We aimed to evaluate the association between rapid sodium correction and ODS in patients with severe hyponatremia.</p><p><strong>Materials and methods: </strong>We searched PubMed, Embase, Scopus, Web of Science, and Cochrane Central Register of Controlled Trials from inception to November 2023. The primary outcome was ODS and the secondary outcomes were in-hospital mortality and length of hospital stay.</p><p><strong>Results: </strong>We identified 7 cohort studies involving 6,032 adult patients with severe hyponatremia. Twenty-nine patients developed ODS, resulting in an incidence rate of 0.48%. Seventeen patients (61%) had a rapid correction of serum sodium in the first or any 24-hour period of admission. Compared with a limited rate of sodium correction, a rapid rate of sodium correction was associated with an increased risk of ODS (RR, 3.91 [95% CI, 1.17 to 13.04]; I<sup>2</sup> = 44.47%; p = 0.03). However, a rapid rate of sodium correction reduced the risk of in-hospital mortality by approximately 50% (RR, 0.51 [95% CI, 0.39 to 0.66]; I<sup>2</sup> = 0.11%; p < 0.001) and the length of stay by 1.3 days (Mean difference, -1.32 [95% CI, -2.54 to -0.10]; I<sup>2</sup> = 71.47%; p = 0.03).</p><p><strong>Conclusions: </strong>Rapid correction of serum sodium may increase the risk of ODS among patients hospitalized with severe hyponatremia. However, ODS may occur in patients regardless of the rate of serum sodium correction.</p>","PeriodicalId":44227,"journal":{"name":"Journal of Critical Care Medicine","volume":"10 3","pages":"209-212"},"PeriodicalIF":1.7000,"publicationDate":"2024-07-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11295268/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Critical Care Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2478/jccm-2024-0030","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Current guidelines recommend limiting the rate of correction in patients with severe hyponatremia to avoid severe neurologic complications such as osmotic demyelination syndrome (ODS). However, published data have been conflicting. We aimed to evaluate the association between rapid sodium correction and ODS in patients with severe hyponatremia.
Materials and methods: We searched PubMed, Embase, Scopus, Web of Science, and Cochrane Central Register of Controlled Trials from inception to November 2023. The primary outcome was ODS and the secondary outcomes were in-hospital mortality and length of hospital stay.
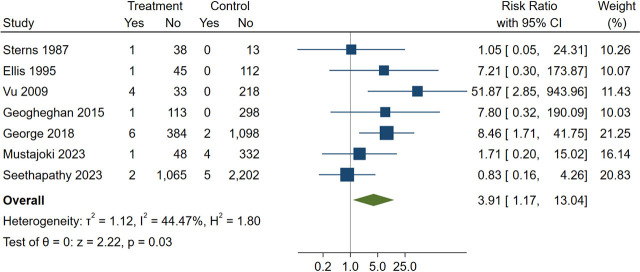
Results: We identified 7 cohort studies involving 6,032 adult patients with severe hyponatremia. Twenty-nine patients developed ODS, resulting in an incidence rate of 0.48%. Seventeen patients (61%) had a rapid correction of serum sodium in the first or any 24-hour period of admission. Compared with a limited rate of sodium correction, a rapid rate of sodium correction was associated with an increased risk of ODS (RR, 3.91 [95% CI, 1.17 to 13.04]; I2 = 44.47%; p = 0.03). However, a rapid rate of sodium correction reduced the risk of in-hospital mortality by approximately 50% (RR, 0.51 [95% CI, 0.39 to 0.66]; I2 = 0.11%; p < 0.001) and the length of stay by 1.3 days (Mean difference, -1.32 [95% CI, -2.54 to -0.10]; I2 = 71.47%; p = 0.03).
Conclusions: Rapid correction of serum sodium may increase the risk of ODS among patients hospitalized with severe hyponatremia. However, ODS may occur in patients regardless of the rate of serum sodium correction.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
