{"title":"[Analysis of the unicentric registry of the Infarction Code program: retrospective cohort].","authors":"Otoniel Toledo-Salinas, Saira Sanjuana Gómez-Flores, Ernesto García-Hernández, Verónica Armenta-Pérez, Andrés García-Rincón","doi":"10.5281/zenodo.10278115","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute coronary syndrome (ACS) is the most serious manifestation of coronary heart disease. The Infarction Code (according to its initialism in Spanish, CI: Código Infarto) program aims to improve the care of these patients.</p><p><strong>Objective: </strong>To describe the clinical presentation and outcomes of CI program in a coronary care unit (CCU).</p><p><strong>Material and methods: </strong>A database of a CCU with 5 years of consecutive records was analyzed. Patients diagnosed with ACS were included. The groups with acute myocardial infarction with and without ST-segment elevation were compared using Student's t, Mann-Whitney U and chi-squared tests. We calculated the relative risk (RR) and 95% confidence intervals (95% CI) of cardiovascular risk factors for mortality.</p><p><strong>Results: </strong>A total of 4678 subjects were analyzed, 78.7% men, mean age 63 years (± 10.7). 80.76% presented acute myocardial infarction with positive ST-segment elevation and fibrinolytic was granted in 60.8% of cases. Percutaneous coronary intervention was performed in 81.4% of patients, which was successful in 82.5% of events. Patients classified as CI presented mortality of 6.8% vs. 11.7%, p = 0.001. Invasive mechanical ventilation had an RR of 26.58 (95% CI: 20.61-34.3) and circulatory shock an RR of 20.86 (95% CI: 16.16-26.93).</p><p><strong>Conclusions: </strong>The CI program decreased mortality by 4.9%. Early fibrinolysis and successful coronary angiography are protective factors for mortality within CCU.</p>","PeriodicalId":94200,"journal":{"name":"Revista medica del Instituto Mexicano del Seguro Social","volume":"62 1","pages":"1-8"},"PeriodicalIF":0.0000,"publicationDate":"2024-01-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12094798/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Revista medica del Instituto Mexicano del Seguro Social","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5281/zenodo.10278115","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Acute coronary syndrome (ACS) is the most serious manifestation of coronary heart disease. The Infarction Code (according to its initialism in Spanish, CI: Código Infarto) program aims to improve the care of these patients.
Objective: To describe the clinical presentation and outcomes of CI program in a coronary care unit (CCU).
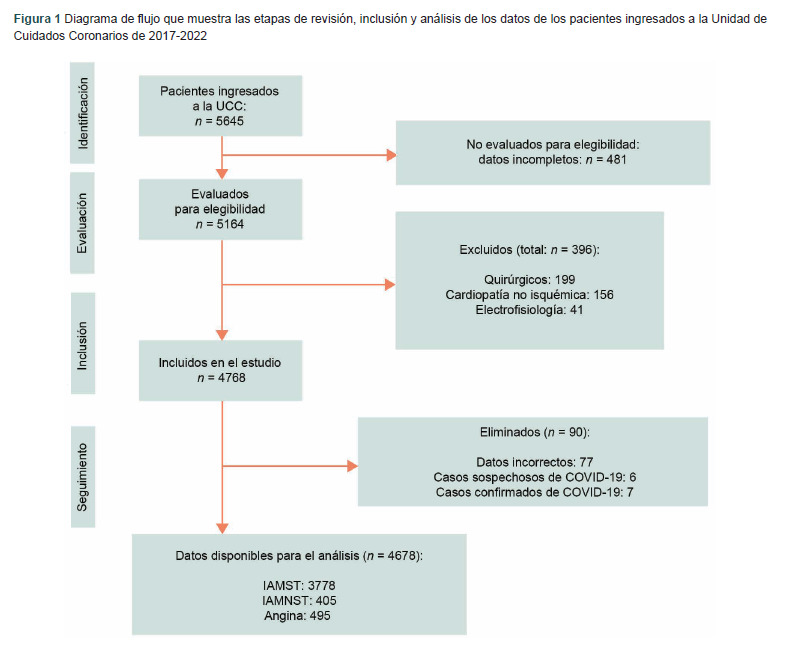
Material and methods: A database of a CCU with 5 years of consecutive records was analyzed. Patients diagnosed with ACS were included. The groups with acute myocardial infarction with and without ST-segment elevation were compared using Student's t, Mann-Whitney U and chi-squared tests. We calculated the relative risk (RR) and 95% confidence intervals (95% CI) of cardiovascular risk factors for mortality.
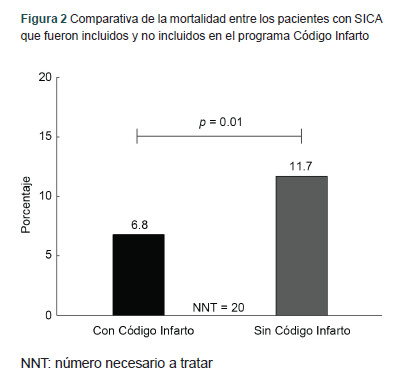
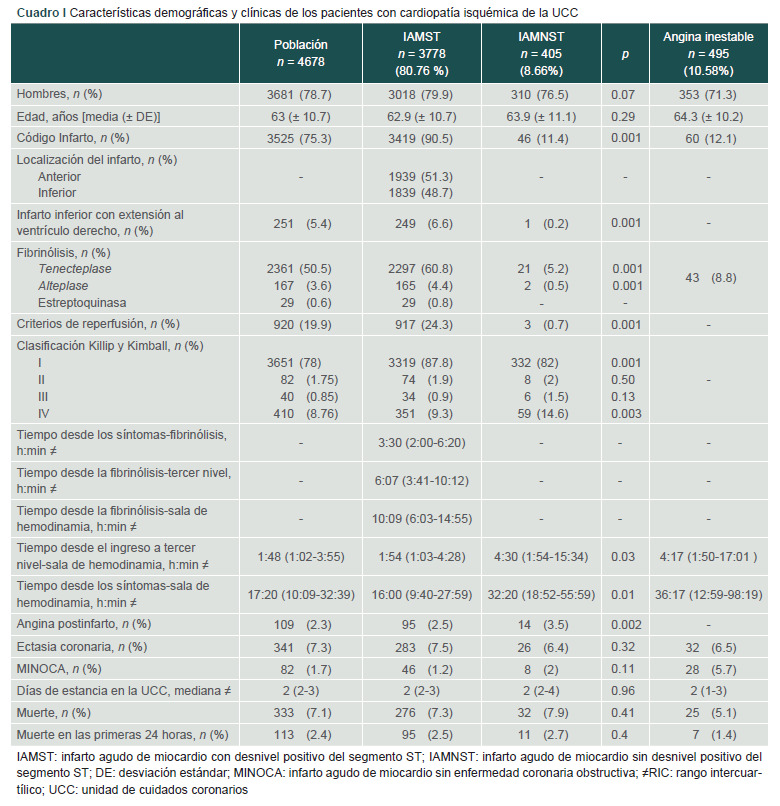
Results: A total of 4678 subjects were analyzed, 78.7% men, mean age 63 years (± 10.7). 80.76% presented acute myocardial infarction with positive ST-segment elevation and fibrinolytic was granted in 60.8% of cases. Percutaneous coronary intervention was performed in 81.4% of patients, which was successful in 82.5% of events. Patients classified as CI presented mortality of 6.8% vs. 11.7%, p = 0.001. Invasive mechanical ventilation had an RR of 26.58 (95% CI: 20.61-34.3) and circulatory shock an RR of 20.86 (95% CI: 16.16-26.93).
Conclusions: The CI program decreased mortality by 4.9%. Early fibrinolysis and successful coronary angiography are protective factors for mortality within CCU.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
