Comparison of analgesic efficacy of combined external oblique intercostal and rectus sheath block with local infiltration analgesia at port site in patients undergoing laparoscopic cholecystectomy: a randomized controlled trial.
{"title":"Comparison of analgesic efficacy of combined external oblique intercostal and rectus sheath block with local infiltration analgesia at port site in patients undergoing laparoscopic cholecystectomy: a randomized controlled trial.","authors":"Vaishnovi Gangadhar, Anju Gupta, Suman Saini","doi":"10.17085/apm.24002","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Conventional fascial plane block approaches for upper abdominal surgeries spare the lateral cutaneous nerve. An external oblique intercostal block (EOIB) may be suitable for upper abdominal incisions as it blocks the lateral and anterior branches of the intercostal nerves T6-T10. However, there is a paucity of studies evaluating this block in clinical settings. The study aimed to compare the analgesic efficacy of combined EOIB and rectus sheath block with local infiltration analgesia (LIA) in laparoscopic cholecystectomy (LC).</p><p><strong>Methods: </strong>After obtaining written informed consent, 70 patients were randomly allocated to undergo right-sided EOIB with 20 ml and left-sided RSB with 10 ml of 0.25% bupivacaine at the end of surgery (group ER, n = 35). Patients in the LIA group (n = 35) underwent local infiltration at the port site using 20 ml of the same solution (group LIA, n=35).</p><p><strong>Results: </strong>The visual analog scale scores with combined EOI and RSB were significantly lower than those with LIA at 1, 2, 4, 8, and 12 h (P < 0.001). Rescue analgesics were required by 65.7% and 14.3% of the patients in the LIA and block groups, respectively (P < 0.001). The time to first rescue analgesic was significantly greater in the ER group than that in the LIA group (2.8 ± 1.10 vs. 1.6 ± 0.50 h; P = 0.012). The number of times rescue analgesia was required was significantly lower in the ER group than that in the LIA group (1.00 ± 0.00 vs. 1.83 ± 0.72; P = 0.015). Nausea and vomiting scores were higher in the LIA group than those in the ER group (P < 0.001). Patient satisfaction scores were higher in the ER group than those in the LIA group.</p><p><strong>Conclusions: </strong>EOIB combined with RSB provides superior analgesia compared with LIA and should be considered for LC.</p>","PeriodicalId":101360,"journal":{"name":"Anesthesia and pain medicine","volume":"19 3","pages":"247-255"},"PeriodicalIF":3.2000,"publicationDate":"2024-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11317318/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and pain medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.17085/apm.24002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/31 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
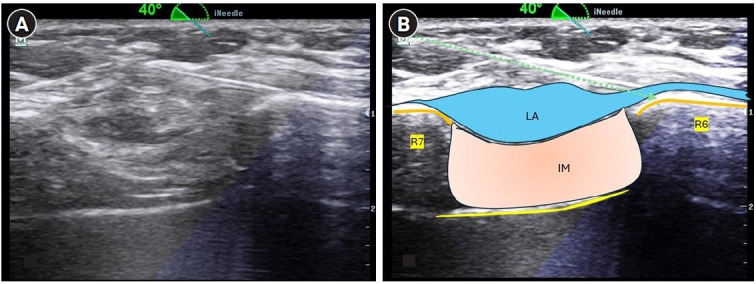
Background: Conventional fascial plane block approaches for upper abdominal surgeries spare the lateral cutaneous nerve. An external oblique intercostal block (EOIB) may be suitable for upper abdominal incisions as it blocks the lateral and anterior branches of the intercostal nerves T6-T10. However, there is a paucity of studies evaluating this block in clinical settings. The study aimed to compare the analgesic efficacy of combined EOIB and rectus sheath block with local infiltration analgesia (LIA) in laparoscopic cholecystectomy (LC).
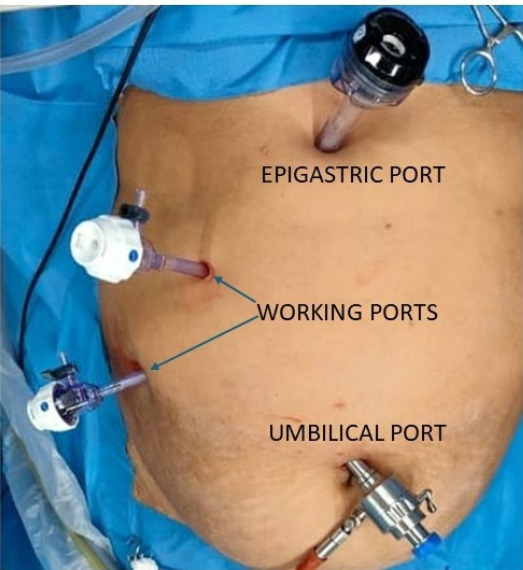
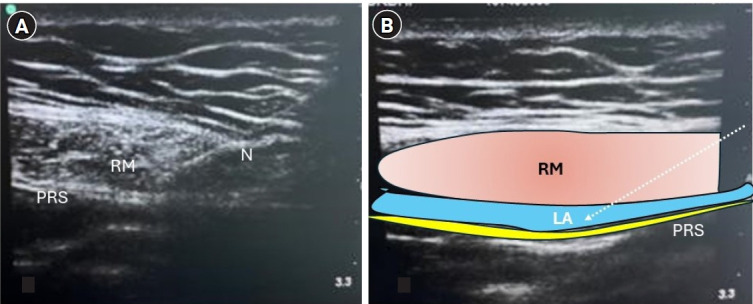
Methods: After obtaining written informed consent, 70 patients were randomly allocated to undergo right-sided EOIB with 20 ml and left-sided RSB with 10 ml of 0.25% bupivacaine at the end of surgery (group ER, n = 35). Patients in the LIA group (n = 35) underwent local infiltration at the port site using 20 ml of the same solution (group LIA, n=35).
Results: The visual analog scale scores with combined EOI and RSB were significantly lower than those with LIA at 1, 2, 4, 8, and 12 h (P < 0.001). Rescue analgesics were required by 65.7% and 14.3% of the patients in the LIA and block groups, respectively (P < 0.001). The time to first rescue analgesic was significantly greater in the ER group than that in the LIA group (2.8 ± 1.10 vs. 1.6 ± 0.50 h; P = 0.012). The number of times rescue analgesia was required was significantly lower in the ER group than that in the LIA group (1.00 ± 0.00 vs. 1.83 ± 0.72; P = 0.015). Nausea and vomiting scores were higher in the LIA group than those in the ER group (P < 0.001). Patient satisfaction scores were higher in the ER group than those in the LIA group.
Conclusions: EOIB combined with RSB provides superior analgesia compared with LIA and should be considered for LC.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
