Joohyung Ha, Jong Cheol Jeong, Jung-Hwa Ryu, Myung-Gyu Kim, Kyu Ha Huh, Kyo Won Lee, Hee-Yeon Jung, Kyung Pyo Kang, Han Ro, Seungyeup Han, Beom Seok Kim, Jaeseok Yang
{"title":"Impact of Arterial Calcification on Cardiovascular and Renal Outcomes in Kidney Transplant Patients.","authors":"Joohyung Ha, Jong Cheol Jeong, Jung-Hwa Ryu, Myung-Gyu Kim, Kyu Ha Huh, Kyo Won Lee, Hee-Yeon Jung, Kyung Pyo Kang, Han Ro, Seungyeup Han, Beom Seok Kim, Jaeseok Yang","doi":"10.1159/000538929","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Coronary artery calcification score (CACS) and abdominal aortic calcification score (AACS) are both well-established markers of vascular stiffness, and previous studies have shown that a higher CACS is a risk factor for chronic kidney disease (CKD) progression. However, the impact of pretransplant CACS and AACS on cardiovascular and renal outcomes in kidney transplant patients has not been established.</p><p><strong>Methods: </strong>We included 944 kidney transplant recipients from the KoreaN cohort study for Outcome in patients With Kidney Transplantation (KNOW-KT) cohort and categorized them into three groups (low, medium, and high) according to baseline CACS (0, 0 < and ≤100, >100) and AACS (0, 1-4, >4). The low (0), medium (0 < and ≤ 100), and high (>100) CACS groups each consisted of 462, 213, and 225 patients, respectively. Similarly, the low (0), medium (1-4), and high (>4) AACS groups included 638, 159, and 147 patients, respectively. The primary outcome was the occurrence of cardiovascular events. The secondary outcomes were all-cause mortality and composite kidney outcomes, which comprised of >50% decline in the estimated glomerular filtration rate and graft loss. Cox regression analysis was used to investigate the association between baseline CACS/AACS and outcomes.</p><p><strong>Results: </strong>The high CACS group (<i>N</i> = 462) faced a significantly higher risk for cardiovascular outcomes (adjusted hazard ratio [aHR], 5.97; 95% confidence interval [CI], 2.01-17.7) and all-cause mortality (aHR, 2.74; 95% CI, 1.27-5.92) compared to the low CACS group (<i>N</i> = 225). Similarly, the high AACS group (<i>N</i> = 638) had an elevated risk for cardiovascular outcomes (aHR, 2.38; 95% CI, 1.16-4.88). Furthermore, the addition of CACS to prediction models improved prediction indices for cardiovascular outcomes. However, the risk of renal outcomes did not differ among CACS or AACS groups.</p><p><strong>Conclusion: </strong>Pretransplant arterial calcification, characterized by high CACS or AACS, is an independent risk factor for cardiovascular outcomes and mortality in kidney transplant patients.</p>","PeriodicalId":17830,"journal":{"name":"Kidney Diseases","volume":"10 4","pages":"249-261"},"PeriodicalIF":3.1000,"publicationDate":"2024-04-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11309755/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Kidney Diseases","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1159/000538929","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Coronary artery calcification score (CACS) and abdominal aortic calcification score (AACS) are both well-established markers of vascular stiffness, and previous studies have shown that a higher CACS is a risk factor for chronic kidney disease (CKD) progression. However, the impact of pretransplant CACS and AACS on cardiovascular and renal outcomes in kidney transplant patients has not been established.
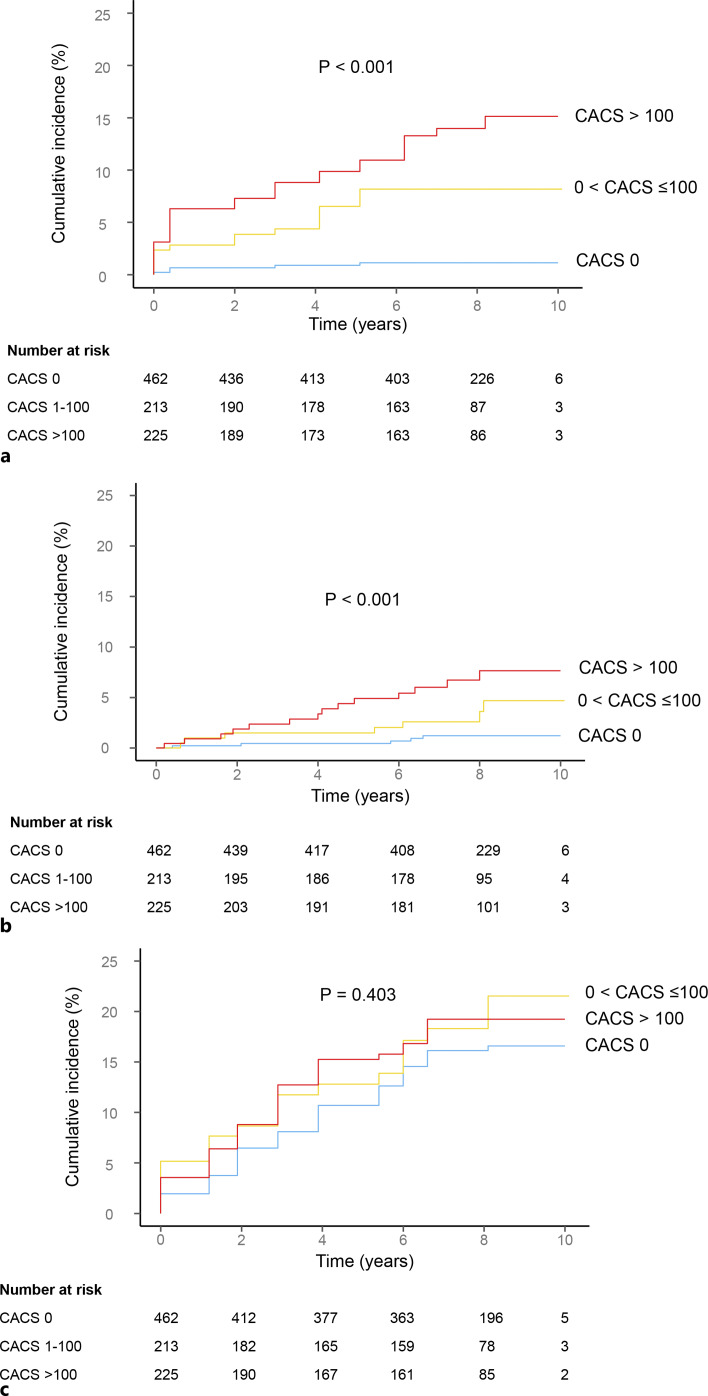
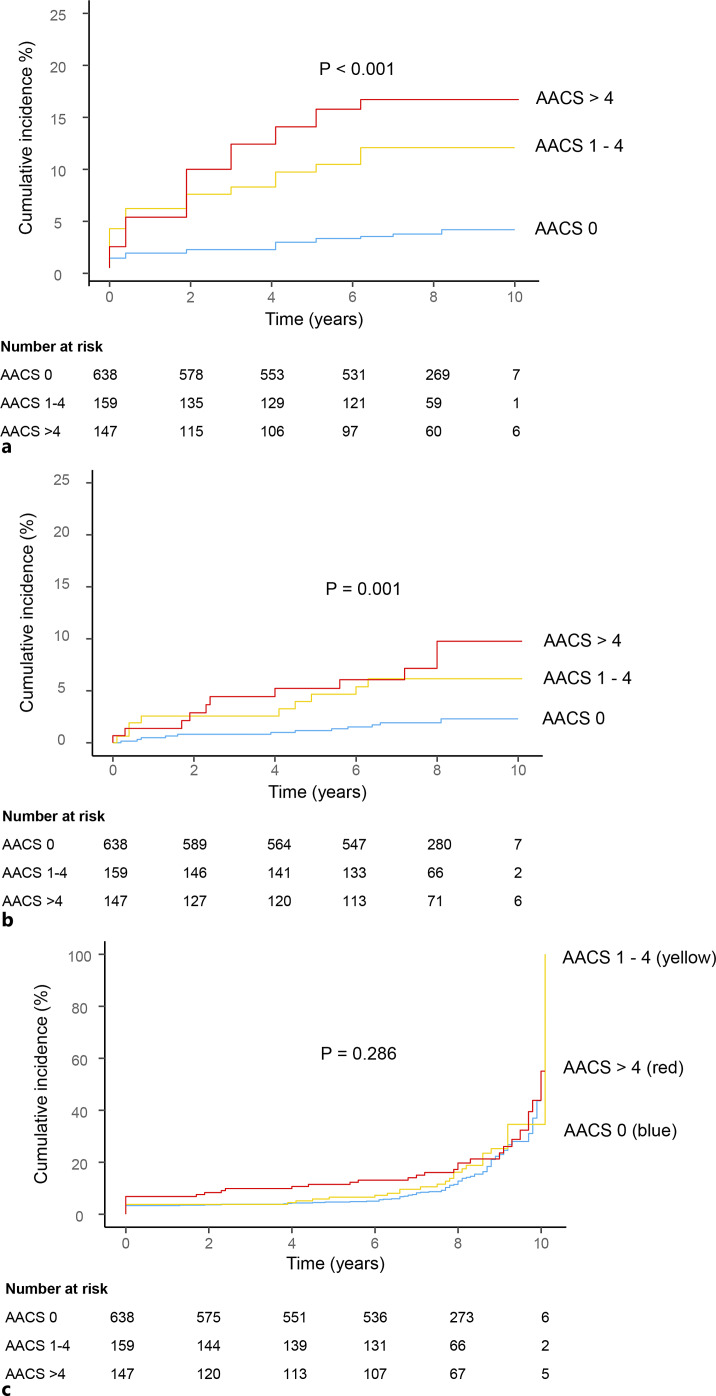
Methods: We included 944 kidney transplant recipients from the KoreaN cohort study for Outcome in patients With Kidney Transplantation (KNOW-KT) cohort and categorized them into three groups (low, medium, and high) according to baseline CACS (0, 0 < and ≤100, >100) and AACS (0, 1-4, >4). The low (0), medium (0 < and ≤ 100), and high (>100) CACS groups each consisted of 462, 213, and 225 patients, respectively. Similarly, the low (0), medium (1-4), and high (>4) AACS groups included 638, 159, and 147 patients, respectively. The primary outcome was the occurrence of cardiovascular events. The secondary outcomes were all-cause mortality and composite kidney outcomes, which comprised of >50% decline in the estimated glomerular filtration rate and graft loss. Cox regression analysis was used to investigate the association between baseline CACS/AACS and outcomes.
Results: The high CACS group (N = 462) faced a significantly higher risk for cardiovascular outcomes (adjusted hazard ratio [aHR], 5.97; 95% confidence interval [CI], 2.01-17.7) and all-cause mortality (aHR, 2.74; 95% CI, 1.27-5.92) compared to the low CACS group (N = 225). Similarly, the high AACS group (N = 638) had an elevated risk for cardiovascular outcomes (aHR, 2.38; 95% CI, 1.16-4.88). Furthermore, the addition of CACS to prediction models improved prediction indices for cardiovascular outcomes. However, the risk of renal outcomes did not differ among CACS or AACS groups.
Conclusion: Pretransplant arterial calcification, characterized by high CACS or AACS, is an independent risk factor for cardiovascular outcomes and mortality in kidney transplant patients.
期刊介绍:
''Kidney Diseases'' aims to provide a platform for Asian and Western research to further and support communication and exchange of knowledge. Review articles cover the most recent clinical and basic science relevant to the entire field of nephrological disorders, including glomerular diseases, acute and chronic kidney injury, tubulo-interstitial disease, hypertension and metabolism-related disorders, end-stage renal disease, and genetic kidney disease. Special articles are prepared by two authors, one from East and one from West, which compare genetics, epidemiology, diagnosis methods, and treatment options of a disease.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
