Malte Ziemann, Monika Lindemann, Michael Hallensleben, Wolfgang Altermann, Karina Althaus, Klemens Budde, Gunilla Einecke, Ute Eisenberger, Andrea Ender, Thorsten Feldkamp, Florian Grahammer, Martina Guthoff, Christopher Holzmann-Littig, Christian Hugo, Teresa Kauke, Stephan Kemmner, Martina Koch, Nils Lachmann, Matthias Marget, Christian Morath, Martin Nitschke, Lutz Renders, Sabine Scherer, Julian Stumpf, Vedat Schwenger, Florian Sommer, Bernd Spriewald, Caner Süsal, Daniel Zecher, Falko M Heinemann, Murielle Verboom
{"title":"Risk Stratification Before Living Donor Kidney Transplantation in Patients With Preformed Donor-specific Antibodies by Different Crossmatch Methods.","authors":"Malte Ziemann, Monika Lindemann, Michael Hallensleben, Wolfgang Altermann, Karina Althaus, Klemens Budde, Gunilla Einecke, Ute Eisenberger, Andrea Ender, Thorsten Feldkamp, Florian Grahammer, Martina Guthoff, Christopher Holzmann-Littig, Christian Hugo, Teresa Kauke, Stephan Kemmner, Martina Koch, Nils Lachmann, Matthias Marget, Christian Morath, Martin Nitschke, Lutz Renders, Sabine Scherer, Julian Stumpf, Vedat Schwenger, Florian Sommer, Bernd Spriewald, Caner Süsal, Daniel Zecher, Falko M Heinemann, Murielle Verboom","doi":"10.1097/TXD.0000000000001680","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Preformed donor-specific HLA antibodies (DSA) are a well-known risk factor in kidney transplantation. There is still considerable debate, however, about the optimal risk stratification among patients with preformed DSA. Additionally, data on the prognostic value of different crossmatch assays in DSA-positive patients are scarce.</p><p><strong>Methods: </strong>DSA-positive living kidney transplant recipients were selected from a multicenter study examining 4233 consecutive renal transplants. An additional 7 patients from 2 further centers were included. Flow cytometric crossmatches (FXM), Luminex-based crossmatches, and virtual crossmatches based on C1q- and C3d-binding antibodies (C1qXM and C3dXM) were performed retrospectively using pretransplant sera and lymphocytes isolated from fresh samples. These samples were obtained from 44 donor and recipient pairs from 12 centers. Clinical outcome data and the control group without DSA were compiled from the previous study and were supplemented by data on 10-y death-censored graft survival (10yGS).</p><p><strong>Results: </strong>Between 19% (C3dXM) and 46% (FXM) of crossmatches were positive. Crossmatch-positive patients showed high incidences of antibody-mediated rejection (AMR) within 6 mo (up to 60% in B-cell FXM+ patients). The incidence of AMR in crossmatch-negative patients ranged between 5% (FXM-) and 13% (C1qXM-). 10yGS was significantly impaired in patients with positive T-cell FXM and total FXM compared with both patients without DSA and those with DSA with negative FXM.</p><p><strong>Conclusions: </strong>Especially FXM are useful for risk stratification, as the outcome of DSA-positive, FXM-negative patients is similar to that of DSA-negative patients, whereas FXM-positive patients have both more AMR and decreased 10yGS. Because of their lower sensitivity, the significance of Luminex-based crossmatches, C1qXM, and C3dXM would have to be examined in patients with stronger DSA.</p>","PeriodicalId":23225,"journal":{"name":"Transplantation Direct","volume":"10 9","pages":"e1680"},"PeriodicalIF":1.9000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11315586/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Transplantation Direct","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/TXD.0000000000001680","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"TRANSPLANTATION","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Preformed donor-specific HLA antibodies (DSA) are a well-known risk factor in kidney transplantation. There is still considerable debate, however, about the optimal risk stratification among patients with preformed DSA. Additionally, data on the prognostic value of different crossmatch assays in DSA-positive patients are scarce.
Methods: DSA-positive living kidney transplant recipients were selected from a multicenter study examining 4233 consecutive renal transplants. An additional 7 patients from 2 further centers were included. Flow cytometric crossmatches (FXM), Luminex-based crossmatches, and virtual crossmatches based on C1q- and C3d-binding antibodies (C1qXM and C3dXM) were performed retrospectively using pretransplant sera and lymphocytes isolated from fresh samples. These samples were obtained from 44 donor and recipient pairs from 12 centers. Clinical outcome data and the control group without DSA were compiled from the previous study and were supplemented by data on 10-y death-censored graft survival (10yGS).
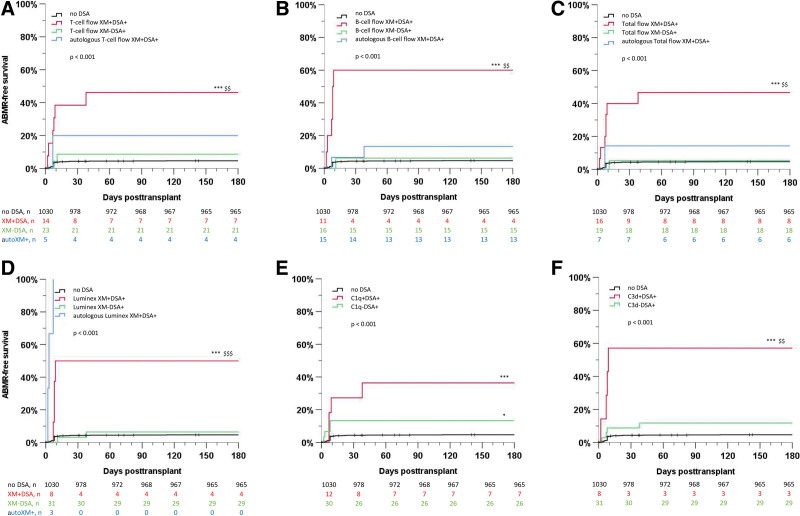
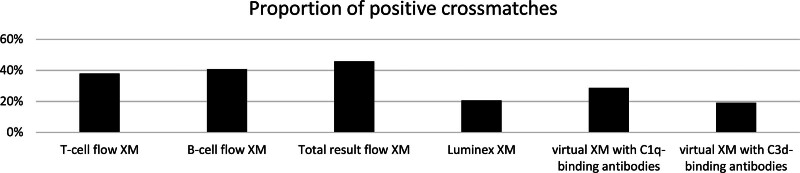
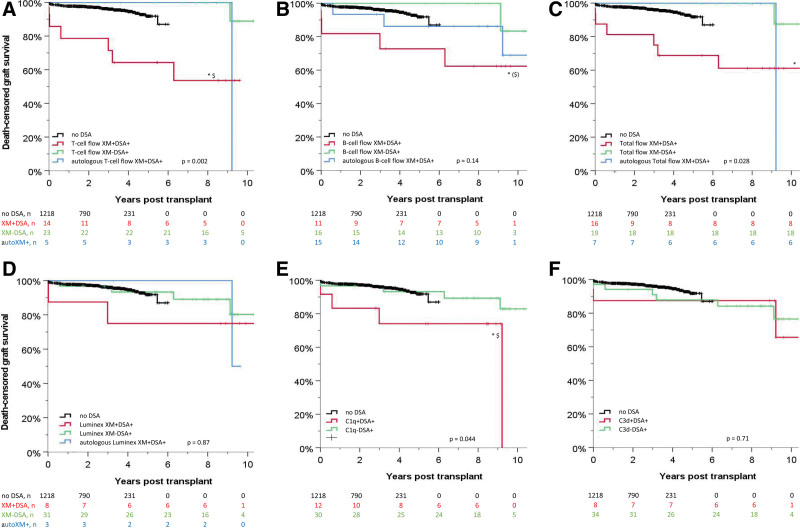
Results: Between 19% (C3dXM) and 46% (FXM) of crossmatches were positive. Crossmatch-positive patients showed high incidences of antibody-mediated rejection (AMR) within 6 mo (up to 60% in B-cell FXM+ patients). The incidence of AMR in crossmatch-negative patients ranged between 5% (FXM-) and 13% (C1qXM-). 10yGS was significantly impaired in patients with positive T-cell FXM and total FXM compared with both patients without DSA and those with DSA with negative FXM.
Conclusions: Especially FXM are useful for risk stratification, as the outcome of DSA-positive, FXM-negative patients is similar to that of DSA-negative patients, whereas FXM-positive patients have both more AMR and decreased 10yGS. Because of their lower sensitivity, the significance of Luminex-based crossmatches, C1qXM, and C3dXM would have to be examined in patients with stronger DSA.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
