Doug A. Gouchoe, Divyaam Satija, Ervin Y. Cui, Dana Ferrari-Light, Matthew C. Henn, Kukbin Choi, Nahush A. Mokadam, Asvin M. Ganapathi, Bryan A. Whitson
{"title":"The impact of ex vivo lung perfusion location on lung transplant outcomes","authors":"Doug A. Gouchoe, Divyaam Satija, Ervin Y. Cui, Dana Ferrari-Light, Matthew C. Henn, Kukbin Choi, Nahush A. Mokadam, Asvin M. Ganapathi, Bryan A. Whitson","doi":"10.1111/aor.14829","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Ex vivo lung perfusion (EVLP) conducted outside of the transplant center has increased in recent years to mitigate its limitation by resources and expertise. We sought to evaluate EVLP performed at transplant centers and externally.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Lung transplant recipients were identified from the United Network for Organ Sharing Database. Recipients were then stratified into two groups based where they were perfused: Transplant Program (TP) or External Perfusion Centers (EPC). The groups were assessed with comparative statistics and long-term survival was assessed by Kaplan–Meier method. The groups were then 1:1 propensity and this process was repeated.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>EPC use was generally restricted to the Southern United States. Following matching, there were no significant differences in post-operative outcomes to include post-operative stroke, dialysis, airway dehiscence, ECMO use, ventilator use or incidence of primary graft dysfunction Grade 3. Adjusted 3-year survival was 68.9% (95% Confidence Interval [CI]: 60.9%–77.9%) for the TP group and 67.6% (95% CI: 61.0%–74.9%) for the EPC group (<i>p</i> = 0.69). In allografts with extended ischemia (14+ h), those in the TP group had significantly longer length of stay, prolonged ventilation and treated rejection in the 1st year, though no significant difference in mid-term survival (<i>p</i> = 0.66).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>EVLP performed at an EPC can be carried out with results and survival similar to allografts undergoing EVLP at a TP. EPCs will extend the valuable resource of EVLP to lung transplant programs without the resources to perform EVLP.</p>\n </section>\n </div>","PeriodicalId":8450,"journal":{"name":"Artificial organs","volume":"48 12","pages":"1467-1475"},"PeriodicalIF":2.3000,"publicationDate":"2024-08-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/aor.14829","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Artificial organs","FirstCategoryId":"5","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/aor.14829","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"ENGINEERING, BIOMEDICAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
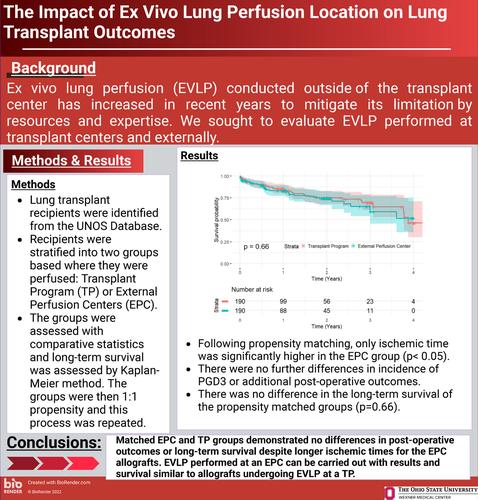
Ex vivo lung perfusion (EVLP) conducted outside of the transplant center has increased in recent years to mitigate its limitation by resources and expertise. We sought to evaluate EVLP performed at transplant centers and externally.
Methods
Lung transplant recipients were identified from the United Network for Organ Sharing Database. Recipients were then stratified into two groups based where they were perfused: Transplant Program (TP) or External Perfusion Centers (EPC). The groups were assessed with comparative statistics and long-term survival was assessed by Kaplan–Meier method. The groups were then 1:1 propensity and this process was repeated.
Results
EPC use was generally restricted to the Southern United States. Following matching, there were no significant differences in post-operative outcomes to include post-operative stroke, dialysis, airway dehiscence, ECMO use, ventilator use or incidence of primary graft dysfunction Grade 3. Adjusted 3-year survival was 68.9% (95% Confidence Interval [CI]: 60.9%–77.9%) for the TP group and 67.6% (95% CI: 61.0%–74.9%) for the EPC group (p = 0.69). In allografts with extended ischemia (14+ h), those in the TP group had significantly longer length of stay, prolonged ventilation and treated rejection in the 1st year, though no significant difference in mid-term survival (p = 0.66).
Conclusion
EVLP performed at an EPC can be carried out with results and survival similar to allografts undergoing EVLP at a TP. EPCs will extend the valuable resource of EVLP to lung transplant programs without the resources to perform EVLP.
期刊介绍:
Artificial Organs is the official peer reviewed journal of The International Federation for Artificial Organs (Members of the Federation are: The American Society for Artificial Internal Organs, The European Society for Artificial Organs, and The Japanese Society for Artificial Organs), The International Faculty for Artificial Organs, the International Society for Rotary Blood Pumps, The International Society for Pediatric Mechanical Cardiopulmonary Support, and the Vienna International Workshop on Functional Electrical Stimulation. Artificial Organs publishes original research articles dealing with developments in artificial organs applications and treatment modalities and their clinical applications worldwide. Membership in the Societies listed above is not a prerequisite for publication. Articles are published without charge to the author except for color figures and excess page charges as noted.





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
