Ying Hu MD, PhD, Bangwu Chen MD, Xiaoyan Wang MD, Shuqi Zhu MD, Shuting Bao MD, Junjun Lu MD, Liyuan Wang MD, Wei Wang MD, PhD, Chenxi Wu MD, Linglu Qi MD, Yan Wang MD, Fan Li MD, Wenjing Xie MD, Yihui Wu MD, Luyao Hu MD, Yizhe Xia MD, Benben Lou MD, Ruoqian Guo MD, Biao Xie MD, Xiaolu Chen MD, Zhaoxia Liang MD, PhD
{"title":"Association between timing of labor induction and neonatal and maternal outcomes: an observational study from China","authors":"Ying Hu MD, PhD, Bangwu Chen MD, Xiaoyan Wang MD, Shuqi Zhu MD, Shuting Bao MD, Junjun Lu MD, Liyuan Wang MD, Wei Wang MD, PhD, Chenxi Wu MD, Linglu Qi MD, Yan Wang MD, Fan Li MD, Wenjing Xie MD, Yihui Wu MD, Luyao Hu MD, Yizhe Xia MD, Benben Lou MD, Ruoqian Guo MD, Biao Xie MD, Xiaolu Chen MD, Zhaoxia Liang MD, PhD","doi":"10.1016/j.ajogmf.2024.101456","DOIUrl":null,"url":null,"abstract":"<div><h3>BACKGROUND</h3><p>Growing evidence suggests that elective induction of labor at 39 weeks’ gestation may lead to more favorable perinatal outcomes than expectant management, however, how to weigh the pros and cons of elective labor induction at 39 weeks, the expectation of spontaneous delivery at 40 or 41 weeks, or delayed labor induction at 40 or 41 weeks on neonatal and maternal outcomes remains a practical challenge in clinical decision-making.</p></div><div><h3>OBJECTIVE</h3><p>We compared the neonatal and maternal outcomes between elective induction of labor at 39 weeks’ gestation and expectant management in a real-world setting. We also divided the expectantly managed group and compared outcomes of the spontaneous delivery at 40 or 41 weeks’ gestation group and the induced group at 40 or 41 weeks’ gestation with those of the elective induction at 39 weeks’ gestation group.</p></div><div><h3>STUDY DESIGN</h3><p>This retrospective cohort study included 21,282 participants who delivered between January 1, 2019, and June 30, 2022. Participants were initially categorized into 3 groups at 39 weeks’ gestation, namely elective induction of labor, spontaneous delivery, and expectant management, for the primary analysis in which elective induction was compared with expectant management. Subsequently, the expectant management group at 39 weeks’ gestation was divided into 3 groups at 40 weeks, and participants who underwent expectant management at 40 weeks were then divided into 2 groups at 41 weeks’ gestation, namely elective induction and spontaneous delivery. In total, 6 groups were compared in the secondary analysis with the elective induction at 39 weeks’ gestation group serving as the reference group.</p></div><div><h3>RESULTS</h3><p>At 39 weeks’ gestational age, participants who underwent elective induction of labor had a significantly lower risk for the primary composite outcomes than participants who were managed expectantly (adjusted odds ratio, 0.72; 95% confidence interval, 0.55–0.95), and there was no significant difference in the risk for cesarean delivery between the 2 groups. After further dividing the expectantly managed group and comparing them with participants who underwent elective induction of labor at 39 weeks’ gestation, those who underwent spontaneous delivery at 40 weeks’ gestation had significantly lower risks for cesarean delivery (0.61; 0.52–0.71) and chorioamnionitis (0.78; 0.61–1.00) but a higher risk for fetal distress (1.39; 1.22–1.57); those with spontaneous delivery at 41 weeks’ gestation had a significantly higher risk for fetal distress (1.44; 1.16–1.79), postpartum hemorrhage (1.83; 1.26–2.66), and prolonged or arrested labor (1.61; 1.02–2.54). Moreover, when compared with participants who underwent elective induction of labor at 39 weeks’ gestation, participants who were induced later in gestation had significantly higher risks for adverse neonatal and maternal outcomes, especially at 40 weeks’ gestation.</p></div><div><h3>CONCLUSION</h3><p>Our findings indicate that elective induction of labor at 39 weeks’ gestation was significantly associated with lower risks for adverse short-term neonatal and maternal outcomes when compared with expectant management. Moreover, our study highlights the nuanced trade-offs in risks and benefits between elective induction at 39 weeks’ gestation and waiting for spontaneous labor or delayed induction at 40 or 41 weeks’ gestation, thus providing valuable insights for clinical decision-making in practice.</p></div>","PeriodicalId":36186,"journal":{"name":"American Journal of Obstetrics & Gynecology Mfm","volume":"6 10","pages":"Article 101456"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.sciencedirect.com/science/article/pii/S2589933324001824/pdfft?md5=29537b27d3b78110d82e0f9bdb84dd71&pid=1-s2.0-S2589933324001824-main.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Obstetrics & Gynecology Mfm","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2589933324001824","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/15 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
BACKGROUND
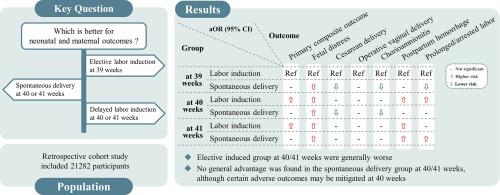
Growing evidence suggests that elective induction of labor at 39 weeks’ gestation may lead to more favorable perinatal outcomes than expectant management, however, how to weigh the pros and cons of elective labor induction at 39 weeks, the expectation of spontaneous delivery at 40 or 41 weeks, or delayed labor induction at 40 or 41 weeks on neonatal and maternal outcomes remains a practical challenge in clinical decision-making.
OBJECTIVE
We compared the neonatal and maternal outcomes between elective induction of labor at 39 weeks’ gestation and expectant management in a real-world setting. We also divided the expectantly managed group and compared outcomes of the spontaneous delivery at 40 or 41 weeks’ gestation group and the induced group at 40 or 41 weeks’ gestation with those of the elective induction at 39 weeks’ gestation group.
STUDY DESIGN
This retrospective cohort study included 21,282 participants who delivered between January 1, 2019, and June 30, 2022. Participants were initially categorized into 3 groups at 39 weeks’ gestation, namely elective induction of labor, spontaneous delivery, and expectant management, for the primary analysis in which elective induction was compared with expectant management. Subsequently, the expectant management group at 39 weeks’ gestation was divided into 3 groups at 40 weeks, and participants who underwent expectant management at 40 weeks were then divided into 2 groups at 41 weeks’ gestation, namely elective induction and spontaneous delivery. In total, 6 groups were compared in the secondary analysis with the elective induction at 39 weeks’ gestation group serving as the reference group.
RESULTS
At 39 weeks’ gestational age, participants who underwent elective induction of labor had a significantly lower risk for the primary composite outcomes than participants who were managed expectantly (adjusted odds ratio, 0.72; 95% confidence interval, 0.55–0.95), and there was no significant difference in the risk for cesarean delivery between the 2 groups. After further dividing the expectantly managed group and comparing them with participants who underwent elective induction of labor at 39 weeks’ gestation, those who underwent spontaneous delivery at 40 weeks’ gestation had significantly lower risks for cesarean delivery (0.61; 0.52–0.71) and chorioamnionitis (0.78; 0.61–1.00) but a higher risk for fetal distress (1.39; 1.22–1.57); those with spontaneous delivery at 41 weeks’ gestation had a significantly higher risk for fetal distress (1.44; 1.16–1.79), postpartum hemorrhage (1.83; 1.26–2.66), and prolonged or arrested labor (1.61; 1.02–2.54). Moreover, when compared with participants who underwent elective induction of labor at 39 weeks’ gestation, participants who were induced later in gestation had significantly higher risks for adverse neonatal and maternal outcomes, especially at 40 weeks’ gestation.
CONCLUSION
Our findings indicate that elective induction of labor at 39 weeks’ gestation was significantly associated with lower risks for adverse short-term neonatal and maternal outcomes when compared with expectant management. Moreover, our study highlights the nuanced trade-offs in risks and benefits between elective induction at 39 weeks’ gestation and waiting for spontaneous labor or delayed induction at 40 or 41 weeks’ gestation, thus providing valuable insights for clinical decision-making in practice.
期刊介绍:
The American Journal of Obstetrics and Gynecology (AJOG) is a highly esteemed publication with two companion titles. One of these is the American Journal of Obstetrics and Gynecology Maternal-Fetal Medicine (AJOG MFM), which is dedicated to the latest research in the field of maternal-fetal medicine, specifically concerning high-risk pregnancies. The journal encompasses a wide range of topics, including:
Maternal Complications: It addresses significant studies that have the potential to change clinical practice regarding complications faced by pregnant women.
Fetal Complications: The journal covers prenatal diagnosis, ultrasound, and genetic issues related to the fetus, providing insights into the management and care of fetal health.
Prenatal Care: It discusses the best practices in prenatal care to ensure the health and well-being of both the mother and the unborn child.
Intrapartum Care: It provides guidance on the care provided during the childbirth process, which is critical for the safety of both mother and baby.
Postpartum Issues: The journal also tackles issues that arise after childbirth, focusing on the postpartum period and its implications for maternal health. AJOG MFM serves as a reliable forum for peer-reviewed research, with a preference for randomized trials and meta-analyses. The goal is to equip researchers and clinicians with the most current information and evidence-based strategies to effectively manage high-risk pregnancies and to provide the best possible care for mothers and their unborn children.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
