{"title":"Transient synovitis associated with leuprolide depot (Lupron).","authors":"Erica A Steen, Susan A Phillips","doi":"10.1530/EDM-24-0031","DOIUrl":null,"url":null,"abstract":"<p><strong>Summary: </strong>A 6.6-year-old female presented to endocrinology with precocious puberty for evaluation and management. Workup was initiated, and a diagnosis of central precocious puberty was confirmed. A decision was made to initiate pubertal blockade using gonadotropin-releasing hormone agonist (GnRHa) therapy with depot leuprolide acetate injections every 3 months. The patient received the first depot leuprolide acetate injection in the right ventrogluteal area. Six hours following the injection, the patient was reported to be inconsolable in pain, which was localized to the right hip site of the earlier injection and associated with a refusal to ambulate. The pain and discomfort continued to progress over the next 24 h despite an alternating regimen of Tylenol and ibuprofen prompting admission to the emergency department. Vital signs demonstrated a low-grade fever and elevated C-reactive protein. An ultrasound of the right hip demonstrated fluid accumulation within the joint. Over the next week, the patient was unable to walk independently and required assistance for activities of daily living. By 2 weeks after the injection, the pain began to remit, and the patient resumed activities of daily living. Following consultation with allergy, a decision was made to continue GnRHa suppressive therapy with an alternative analog (Triptodur). The patient tolerated subsequent treatment without reaction.</p><p><strong>Learning points: </strong>Although gonadotropin-releasing hormone agonists (GnRHa) have a generally good safety profile, there is a history of both local and systemic hypersensitivity reactions associated with their use. Despite the long-acting formulation of depot leuprolide acetate, the systemic reaction in this case appears to be self-limited. Discontinuation of therapy or a change to an alternative formulation of GnRHa analog should be considered based on the need for therapy versus the potential risk of rechallenge.</p>","PeriodicalId":37467,"journal":{"name":"Endocrinology, Diabetes and Metabolism Case Reports","volume":"2024 3","pages":""},"PeriodicalIF":0.7000,"publicationDate":"2024-08-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11378123/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology, Diabetes and Metabolism Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1530/EDM-24-0031","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/7/1 0:00:00","PubModel":"Print","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
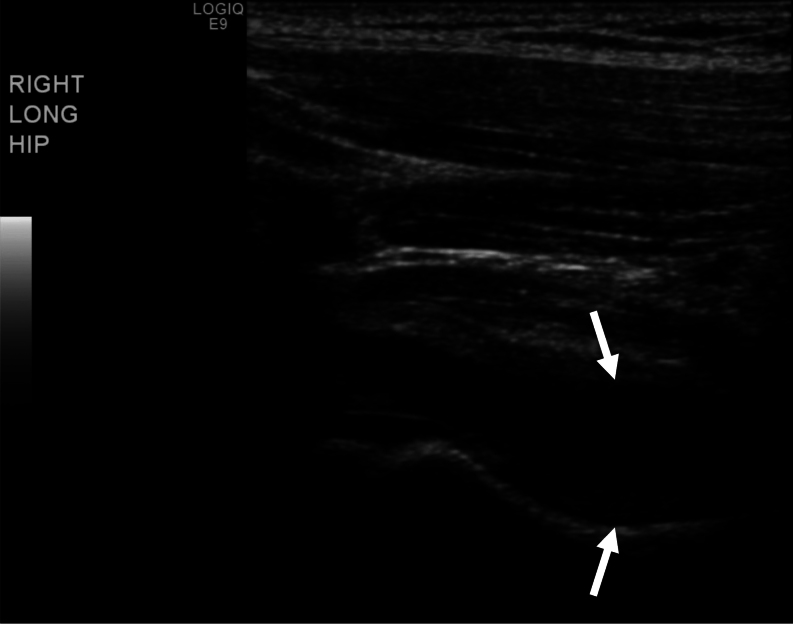
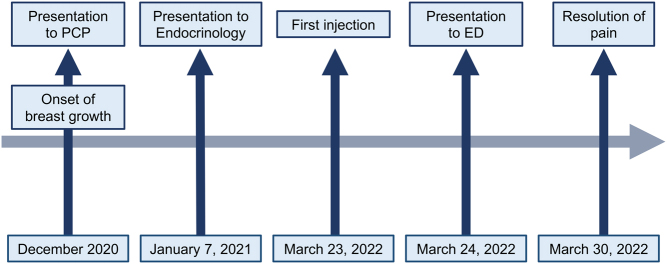
Summary: A 6.6-year-old female presented to endocrinology with precocious puberty for evaluation and management. Workup was initiated, and a diagnosis of central precocious puberty was confirmed. A decision was made to initiate pubertal blockade using gonadotropin-releasing hormone agonist (GnRHa) therapy with depot leuprolide acetate injections every 3 months. The patient received the first depot leuprolide acetate injection in the right ventrogluteal area. Six hours following the injection, the patient was reported to be inconsolable in pain, which was localized to the right hip site of the earlier injection and associated with a refusal to ambulate. The pain and discomfort continued to progress over the next 24 h despite an alternating regimen of Tylenol and ibuprofen prompting admission to the emergency department. Vital signs demonstrated a low-grade fever and elevated C-reactive protein. An ultrasound of the right hip demonstrated fluid accumulation within the joint. Over the next week, the patient was unable to walk independently and required assistance for activities of daily living. By 2 weeks after the injection, the pain began to remit, and the patient resumed activities of daily living. Following consultation with allergy, a decision was made to continue GnRHa suppressive therapy with an alternative analog (Triptodur). The patient tolerated subsequent treatment without reaction.
Learning points: Although gonadotropin-releasing hormone agonists (GnRHa) have a generally good safety profile, there is a history of both local and systemic hypersensitivity reactions associated with their use. Despite the long-acting formulation of depot leuprolide acetate, the systemic reaction in this case appears to be self-limited. Discontinuation of therapy or a change to an alternative formulation of GnRHa analog should be considered based on the need for therapy versus the potential risk of rechallenge.
期刊介绍:
Endocrinology, Diabetes & Metabolism Case Reports publishes case reports on common and rare conditions in all areas of clinical endocrinology, diabetes and metabolism. Articles should include clear learning points which readers can use to inform medical education or clinical practice. The types of cases of interest to Endocrinology, Diabetes & Metabolism Case Reports include: -Insight into disease pathogenesis or mechanism of therapy - Novel diagnostic procedure - Novel treatment - Unique/unexpected symptoms or presentations of a disease - New disease or syndrome: presentations/diagnosis/management - Unusual effects of medical treatment - Error in diagnosis/pitfalls and caveats





 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
