Maria Luisa C. Policarpio-Nicolas, Sydnee Webb, Elizabeth M. Azzato, Rema Rao Chaari, Erika Hissong, Jennifer A. Brainard
{"title":"Cytologic Findings and Ancillary Tests Results of Sclerosing Pneumocytoma: Our Institutional Experience","authors":"Maria Luisa C. Policarpio-Nicolas, Sydnee Webb, Elizabeth M. Azzato, Rema Rao Chaari, Erika Hissong, Jennifer A. Brainard","doi":"10.1002/dc.25396","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Introduction</h3>\n \n <p>Sclerosing pneumocytoma (SP) is a rare benign tumor and a potential diagnostic pitfall. Our aim was to review the cytologic features of our surgically diagnosed SP cases including the clinical, immunohistochemical and available molecular findings.</p>\n </section>\n \n <section>\n \n <h3> Materials and Methods</h3>\n \n <p>A computerized search from 2013 to 2020 for surgical cases with corresponding cytology specimens diagnosed as SP was performed. The clinical data, cytology, and surgical specimens were collated for analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Six cytology specimens were collected. All were female (mean age = 35). Three have incidental lung nodules and three with cough. Cytologic findings showed variable architectural pattern (papillary, solid, singly scattered, acinar/rosette-like) and cellular heterogeneity (surface, stromal, epithelioid, plasmacytoid cells). Atypia was identified in 4/6 cases. The original cytology diagnoses were negative = 1, SP = 2 and adenocarcinoma = 3. The latter diagnoses were amended to SP after review of the surgical specimens. The three false positive cases on review have cytologic features mimicking adenocarcinoma. Immunohistochemical stains showed tumor cells (surface and stromal) were positive for TTF-1, and EMA with only the surface cells positive for pancytokeratin and Napsin A. Though two cases sent for molecular testing were negative for <i>AKT1</i> or <i>CTNNB1</i> exon 3 mutation, our panel did not evaluate <i>AKT1</i> exon 4.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>SP is a diagnostic pitfall with 50% initially misdiagnosed as adenocarcinoma. Integrating the clinical/radiologic findings, cytologic features, and performance of immunohistochemistry on cell block are helpful in avoiding misdiagnosis. Molecular testing for recurrent mutations, if present, could be helpful for diagnosis and possible therapy options. However, routinely used molecular testing may not always capture relevant molecular markers for SP.</p>\n </section>\n </div>","PeriodicalId":11349,"journal":{"name":"Diagnostic Cytopathology","volume":"53 1","pages":"3-9"},"PeriodicalIF":1.0000,"publicationDate":"2024-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/dc.25396","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic Cytopathology","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/dc.25396","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"MEDICAL LABORATORY TECHNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Sclerosing pneumocytoma (SP) is a rare benign tumor and a potential diagnostic pitfall. Our aim was to review the cytologic features of our surgically diagnosed SP cases including the clinical, immunohistochemical and available molecular findings.
Materials and Methods
A computerized search from 2013 to 2020 for surgical cases with corresponding cytology specimens diagnosed as SP was performed. The clinical data, cytology, and surgical specimens were collated for analysis.
Results
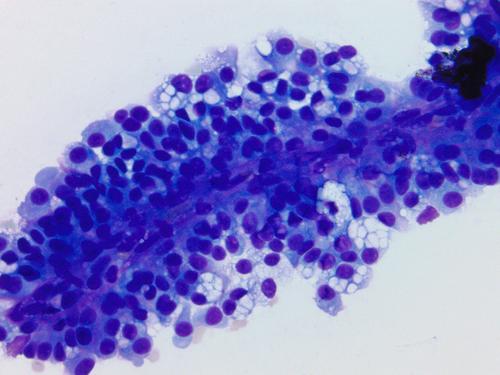
Six cytology specimens were collected. All were female (mean age = 35). Three have incidental lung nodules and three with cough. Cytologic findings showed variable architectural pattern (papillary, solid, singly scattered, acinar/rosette-like) and cellular heterogeneity (surface, stromal, epithelioid, plasmacytoid cells). Atypia was identified in 4/6 cases. The original cytology diagnoses were negative = 1, SP = 2 and adenocarcinoma = 3. The latter diagnoses were amended to SP after review of the surgical specimens. The three false positive cases on review have cytologic features mimicking adenocarcinoma. Immunohistochemical stains showed tumor cells (surface and stromal) were positive for TTF-1, and EMA with only the surface cells positive for pancytokeratin and Napsin A. Though two cases sent for molecular testing were negative for AKT1 or CTNNB1 exon 3 mutation, our panel did not evaluate AKT1 exon 4.
Conclusions
SP is a diagnostic pitfall with 50% initially misdiagnosed as adenocarcinoma. Integrating the clinical/radiologic findings, cytologic features, and performance of immunohistochemistry on cell block are helpful in avoiding misdiagnosis. Molecular testing for recurrent mutations, if present, could be helpful for diagnosis and possible therapy options. However, routinely used molecular testing may not always capture relevant molecular markers for SP.
期刊介绍:
Diagnostic Cytopathology is intended to provide a forum for the exchange of information in the field of cytopathology, with special emphasis on the practical, clinical aspects of the discipline. The editors invite original scientific articles, as well as special review articles, feature articles, and letters to the editor, from laboratory professionals engaged in the practice of cytopathology. Manuscripts are accepted for publication on the basis of scientific merit, practical significance, and suitability for publication in a journal dedicated to this discipline. Original articles can be considered only with the understanding that they have never been published before and that they have not been submitted for simultaneous review to another publication.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
