Khrystia M MacKinnon, Samuel Seshadri, Jonathan F Mailman, Eric Sy
{"title":"Impact of Rounding Checklists on the Outcomes of Patients Admitted to ICUs: A Systematic Review and Meta-Analysis.","authors":"Khrystia M MacKinnon, Samuel Seshadri, Jonathan F Mailman, Eric Sy","doi":"10.1097/CCE.0000000000001140","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To evaluate the effectiveness of ICU rounding checklists on outcomes.</p><p><strong>Data sources: </strong>Five electronic databases (MEDLINE, Embase, CINAHL, Cochrane Library, and Google Scholar) were searched from inception to May 10, 2024.</p><p><strong>Study selection: </strong>Cohort studies, case-control studies, and randomized controlled trials comparing the use of rounding checklists to no checklists were included. Other article types were excluded.</p><p><strong>Data extraction: </strong>The primary outcome was in-hospital mortality. Secondary outcomes included ICU and 30-day mortality; hospital and ICU length of stay (LOS); duration of mechanical ventilation; and frequency of catheter-associated urinary tract infections, central line-associated bloodstream infections (CLABSI), and ventilator-associated pneumonia. Additional outcomes included healthcare provider perceptions of checklists.</p><p><strong>Data synthesis: </strong>Pooled estimates were obtained using an inverse-variance random-effects meta-analysis model. Certainty of evidence was evaluated using Grading of Recommendations Assessment, Development, and Evaluation. There were 30 included studies (including > 32,000 patients) in the review. Using an ICU rounding checklist was associated with reduced in-hospital mortality (risk ratio [RR] 0.80; 95% CI, 0.70-0.92; 12 observational studies; 17,269 patients; I2 = 48%; very low certainty of evidence). The use of an ICU rounding checklist was also associated with reduced ICU mortality (8 observational studies, p = 0.006), 30-day mortality (2 observational studies, p < 0.001), hospital LOS (11 observational studies, p = 0.02), catheter-associated urinary tract infections (CAUTI) (6 observational studies, p = 0.01), and CLABSI (6 observational studies, p = 0.02). Otherwise, there were no significant differences with using ICU rounding checklists on other patient-related outcomes. Healthcare providers' perceptions of checklists were generally positive.</p><p><strong>Conclusions: </strong>The use of an ICU rounding checklist may improve in-hospital mortality, as well as other important patient-related outcomes. However, well-designed randomized studies are necessary to increase the certainty of evidence and determine which elements should be included in an ICU rounding checklist.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"6 8","pages":"e1140"},"PeriodicalIF":2.7000,"publicationDate":"2024-08-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11338257/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001140","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To evaluate the effectiveness of ICU rounding checklists on outcomes.
Data sources: Five electronic databases (MEDLINE, Embase, CINAHL, Cochrane Library, and Google Scholar) were searched from inception to May 10, 2024.
Study selection: Cohort studies, case-control studies, and randomized controlled trials comparing the use of rounding checklists to no checklists were included. Other article types were excluded.
Data extraction: The primary outcome was in-hospital mortality. Secondary outcomes included ICU and 30-day mortality; hospital and ICU length of stay (LOS); duration of mechanical ventilation; and frequency of catheter-associated urinary tract infections, central line-associated bloodstream infections (CLABSI), and ventilator-associated pneumonia. Additional outcomes included healthcare provider perceptions of checklists.
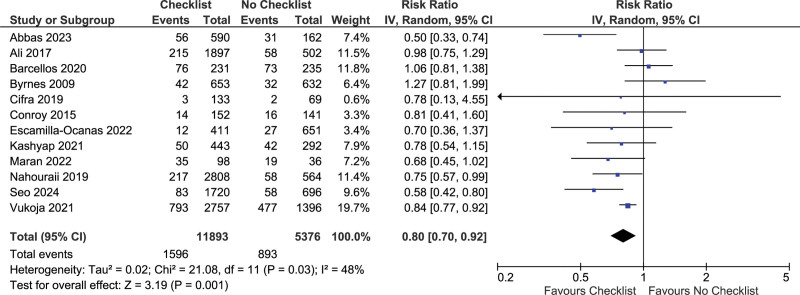
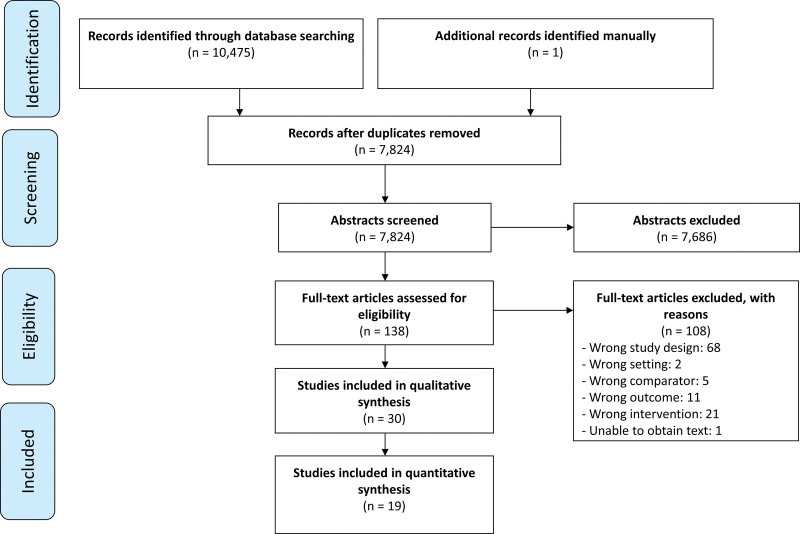
Data synthesis: Pooled estimates were obtained using an inverse-variance random-effects meta-analysis model. Certainty of evidence was evaluated using Grading of Recommendations Assessment, Development, and Evaluation. There were 30 included studies (including > 32,000 patients) in the review. Using an ICU rounding checklist was associated with reduced in-hospital mortality (risk ratio [RR] 0.80; 95% CI, 0.70-0.92; 12 observational studies; 17,269 patients; I2 = 48%; very low certainty of evidence). The use of an ICU rounding checklist was also associated with reduced ICU mortality (8 observational studies, p = 0.006), 30-day mortality (2 observational studies, p < 0.001), hospital LOS (11 observational studies, p = 0.02), catheter-associated urinary tract infections (CAUTI) (6 observational studies, p = 0.01), and CLABSI (6 observational studies, p = 0.02). Otherwise, there were no significant differences with using ICU rounding checklists on other patient-related outcomes. Healthcare providers' perceptions of checklists were generally positive.
Conclusions: The use of an ICU rounding checklist may improve in-hospital mortality, as well as other important patient-related outcomes. However, well-designed randomized studies are necessary to increase the certainty of evidence and determine which elements should be included in an ICU rounding checklist.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
