Surgery for subaxial cervical spine injuries: which is better: anterior, posterior, or anterior-posterior combined approach?: a systematic review and meta-analysis.
Abdul Hafid Bajamal, Eko Agus Subagio, Pandu Wicaksono, I Gusti Made Aswin Rahmadi Ranuh, Muhammad Faris, Budi Utomo
{"title":"Surgery for subaxial cervical spine injuries: which is better: anterior, posterior, or anterior-posterior combined approach?: a systematic review and meta-analysis.","authors":"Abdul Hafid Bajamal, Eko Agus Subagio, Pandu Wicaksono, I Gusti Made Aswin Rahmadi Ranuh, Muhammad Faris, Budi Utomo","doi":"10.31616/asj.2023.0266","DOIUrl":null,"url":null,"abstract":"<p><p>Both anterior and posterior approaches have shown insignificant differences in good clinical outcomes with one over another advantages and disadvantages. This review aimed to provide evidence for the best management of subaxial cervical spine injuries and discuss the clinical outcomes and complications. Clinical studies of anterior versus posterior and anterior versus anterior-posterior (combined) approaches to subaxial cervical spine injury were searched electronically from PubMed, Medline, ScienceDirect, Cochrane Library, and other Internet databases. Clinical improvement, complication rates, and mortality rates showed no significant differences with an odds ratio of 1.09 (95% confidence interval [CI], 0.79-1.49; p=0.61) for the anterior versus posterior approach and an odds ratio of 1.05 (95% CI, 0.35-3.18; p=0.93) for the anterior versus the combined approach. Surgical duration and blood loss were significantly different between the anterior and posterior groups with a mean difference of -42.84 (95% CI, -64.39 to 21.29; p<0.0001); -212.91 (95% CI, -417.60 to 8.22; p=0.04), respectively, whereas the length of hospitalization did not (p=0.16). No difference was found between the groups when compared by clinical improvement and complication rate. Meanwhile, the anterior approach was superior to the posterior approach in terms of surgical duration, blood loss, and hospitalization length.</p>","PeriodicalId":8555,"journal":{"name":"Asian Spine Journal","volume":" ","pages":"594-607"},"PeriodicalIF":2.7000,"publicationDate":"2024-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11366557/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Asian Spine Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.31616/asj.2023.0266","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/8/21 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
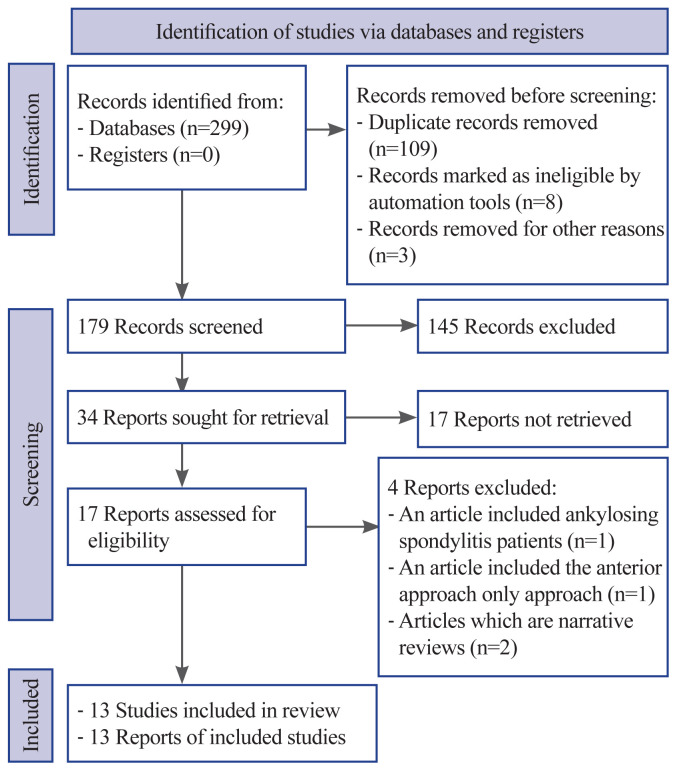
Both anterior and posterior approaches have shown insignificant differences in good clinical outcomes with one over another advantages and disadvantages. This review aimed to provide evidence for the best management of subaxial cervical spine injuries and discuss the clinical outcomes and complications. Clinical studies of anterior versus posterior and anterior versus anterior-posterior (combined) approaches to subaxial cervical spine injury were searched electronically from PubMed, Medline, ScienceDirect, Cochrane Library, and other Internet databases. Clinical improvement, complication rates, and mortality rates showed no significant differences with an odds ratio of 1.09 (95% confidence interval [CI], 0.79-1.49; p=0.61) for the anterior versus posterior approach and an odds ratio of 1.05 (95% CI, 0.35-3.18; p=0.93) for the anterior versus the combined approach. Surgical duration and blood loss were significantly different between the anterior and posterior groups with a mean difference of -42.84 (95% CI, -64.39 to 21.29; p<0.0001); -212.91 (95% CI, -417.60 to 8.22; p=0.04), respectively, whereas the length of hospitalization did not (p=0.16). No difference was found between the groups when compared by clinical improvement and complication rate. Meanwhile, the anterior approach was superior to the posterior approach in terms of surgical duration, blood loss, and hospitalization length.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
